Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
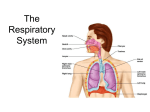
THE RESPIRATORY SYSTEM Air Supply The wind beneath my wings The Length and Breath of it.. • The Anatomy of the Respiratory Tract • Mechanism of Respiratory movements • The measurements of Pulmonary Function Respiratory Organs • Nose and nasal cavities • Pharynx • Larynx • Trachea • Bronchi -2 • Lungs and pleura • Muscles of respiration The Nose Job • This cavity is divided into 2 halves separated by • • • • the Nasal Septum The borders of the cavity are mostly bones of the face and skull with the cartilages anteriorly The cavity leads to the pharynx with their meeting point – the Naso-pharynx. The Para nasal sinuses – maxillary/frontal/sphenoid/Ethmoid , all drain into the nasal cavity. The lining is a vascular mucous membrane made of ciliated columnar epithelium which produces mucous. Functions of the nose • Warming – by high vascularity • Filtering – by hair in nostrils & sticky mucous • Moistening – picked up while flowing over the mucous membrane • Special sense of smell – endings of 1st cranial nerve – olfactory which are exposed by the pores in the cribriform plate (part of Ethmoid bone) Look at your nose- the inside story The Pharynx • It is a tube around 12-14cm long which runs from the base of the skull to the position of the 6th cervical vertebrae. • It is lined by mucous membrane and has a strong smooth muscle layer that helps to propel food into the oesophagus. • This lower end is narrower. Pharynx – the 3 acts Act 1 – Nasopharynx • Nasal part above soft palate • Auditory tubes drain into it • Contains the nasal tonsils (adenoids) that atrophy after age 7. Act 2 - Oropharynx • Oral part • Palatine tonsils – that usually get repeatedly infected due its position. • The Uvula – that separates the oral and nasal cavities during the act of swallowing. Act 3 - Laryngopharynx • The laryngeal part • Composed of mucous membrane layer, fibrous layer and muscle layer Functions of Pharynx • Passage for food and air • Warming and humidifying air • Taste – olfactory nerve ends in wall • Hearing – auditory tube allows sound to enter the middle ear • Protection – lymphatic tissue – the tonsils Larynx • The voice box – extends from tongue to the trachea • Composed of 3 main, different sized cartilages, attached to each other by ligaments. • The smaller cartilages are involved in voice production. Three of the Throat Thyroid • Most prominent, lined by ciliated columnar epithelium – whose function is to produce mucous that traps foreign bodies and propels them upwards. Cricoid • Ring shaped, encircles the larynx supportive role Epiglottis • Responsible for closing the tracheal opening when food is swallowed, to prevent choking. Functions of Larynx • Production of sound – through vibration of vocal cords • Speech • Protection of lower respiratory tract – epiglottis • Passageway for air • Humidifying, warming and filtering of air Trachea • It is the continuation of the larynx beneath the • • • epiglottis. Around 10 cm long and has a series of 16-20 cartilages which share a wall with the oesophagus posteriorly. It ends at around the 5th thoracic vertebra, where it bifurcates into the Left & Right Bronchus- connected to the lung Inner lining of ciliated columnar epithelium which contains mucous producing cells Functions of Trachea Support and patency • The cartilages prevent kinking/obstruction in head/neck movements • As its attached to oesophagus –allows it’s expansion • Prevent collapse during pressure alteration during breathing Mucociliary escalator • Upward movement of cilia make sure the mucous moves upward as it cleans the air. With it being either swallowed or expectorated Also cough reflex on irritation of nerve endings, warming, humidifying and filtering of air. Bronchi and its branches • The right (shorter) divides • • into 3 further lobar branches – lobes of lungs, but only 2 for the left bronchus They then become smaller secondary and even smaller tertiary bronchi Those then divide into smaller bronchioles & Respiratory bronchioles Bronchi and bronchioles • Lined with ciliated columnar epithelium • No cartilage only thick smooth muscle • The lining epithelium changes in bronchiole – cuboidal epithelium Non-breathing functions • Control of air entry by muscle contraction • Warming, support and patency • Cleansing & cough reflex Walls that breathe- the Alveoli • Single layer of squamous epithelium in alveolar ducts and alveoli • Surrounded by network of capillaries with only 1 layer of cells separating- essential exchange of gases • Special chemical – Surfactant, which maintains hydration, reduces surface tension thereby preventing collapse of alveoli during expiration Functions • External respiration • Defence against microbes • Warming and humidifying Lung story • 2, cone shaped, on either side of heart Major markings • Apex – top or supraclavicular • Base – bottom on Diaphragm • Costal surface – front/side, convex, with costal cartilages, intercostal muscles & ribs • Medial surface – inner, concave, with triangular hilum, point of entry/exit of vessels • Hilum- root of lung Look at the Lung Hilum – the passage Structures that enter/exit through the Hilum – for each lung • 1 Bronchus • 1 Pulmonary artery • 2 Pulmonary veins • 1 Bronchial artery • Bronchial veins • Lymph vessels • ANS nerves Pleura • It is a closed sac of serous membrane 2 layers• Visceral Pleura – attached to lung • Parietal Pleura – attached to thoracic cavity • Space in between – pleural cavity containing serous fluid – which allows frictionless gliding of layers over each other during respiration • Serous fluid secreted by epithelial cells of pleura and its puncture would lead to collapsed lung. Intercostal muscles • Attached between Ribs • Their contraction and • • expansion allow for rib movement, increasing and decreasing thoracic volume Types- internal and external Allow the rib cage to increase in size laterally, anterioposteriorly and vertically Diaphragm • Dome shaped with central tendon- attached to lower ribs. • Moves upward in expiration and downwards in inspiration • Nerve supply – Phrenic Nerve Composition of Air • Each gas has its own partial pressure • • • • • • Nitrogen Oxygen Carbon-dioxide Water vapour Inert gases • • corresponding to its proportion The composition of alveolar air is constant, contains more CO2 and less O2 Gas exchange between the blood and alveoli is continuous and independent of the respiratory cycle Dead space 150 ml of air – mix of alveolar and atmospheric air Respiration – Gas Exchange • The exchange occurs • • when there is a difference in the partial pressures, across a semi-permeable membrane Gases always move from high to low concentration until equilibrium Aided by huge surface area of membrane and slow flow of blood External respiration • Exchange between the alveoli and blood. CO2 moves from high conc. in capillary to alveoli and opposite for O2 Internal respiration • Exchange between blood and body cells. O2 moves from high conc. in blood to low in cells and opposite for CO2 Pulmonary Function • Pulmonary function tests - a broad range of tests • that measure how well the lungs take in and exhale air and how efficiently they transfer oxygen into the blood. Spirometer - measures how well the lungs exhale. The information gathered during this test is useful in diagnosing certain types of lung disorders, but is most useful when assessing for obstructive lung diseases (especially asthma and chronic obstructive pulmonary disease, COPD). Lung function Measurement Terminology and Definitions • FVC - Forced Vital Capacity - after the patient has taken in the deepest possible breath, this is the volume of air which can be forcibly and maximally exhaled out of the lungs until no more can be expired. FVC is usually expressed in units called liters. This PFT value is critically important in the diagnosis of obstructive and restrictive diseases. • FEV1 - Forced Expiratory Volume in One Second this is the volume of air which can be forcibly exhaled from the lungs in the first second of a forced expiratory maneuver. It is expressed as liters. This PFT value is critically important in the diagnosis of obstructive and restrictive diseases. • PEFR - Peak Expiratory Flow Rate - this is maximum • flow rate achieved by the patient during the forced vital capacity maneuver beginning after full inspiration and starting and ending with maximal expiration - it can either be measured in L/sec or L/min - this is a useful measure to see if the treatment is improving obstructive diseases like broncho-constriction secondary to asthma. FEF - Forced Expiratory Flow - Forced expiratory Flow is a measure of how much air can be expired from the lungs. It is a flow rate measurement. It is measured as liters/second or liters/minute. The FVC expiratory curve is divided into quartiles and therefore there is a FEF that exists for each quartile. The quartiles are expressed as FEF25%, FEF50%, and FEF75% of FVC. • MVV - Maximal Voluntary Ventilation - this value is determined by having the patient breathe in and out as rapidly and fully as possible for 12 -15 seconds - the total volume of air moved during the test can be expressed as L/sec or L/min - this test parameter reflects the status of the respiratory muscles, compliance of the thorax-lung complex, and airway resistance. Surgeons like this test value because it is a quick and easy way to assess the strength of the patient's pulmonary musculature prior to surgery. MVV can therefore be viewed as a measure of respiratory muscle strength. One major cautionary note is that this test is effort dependent and therefore can be a poor predictor of true pulmonary strength and compliance. BREATHE IN… BREATHE OUT…….! Dr Anjali Hariharan