Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
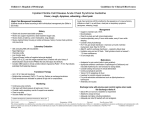
Hematocrit During the Cardiopulmonary Bypass: Impact on Clinical Outcome During Ascending Aortic Surgery SF Zhou MD1, AL. Estrera MD2, T Pawelek MD1, C Ignacio MD1, S Panthayi MD1, MD; K Shebaclo BS1, H Safi MD2, R Sheinbaum MD1 Department of Anesthesia1 Department of Cardiothoracic and Vascular Surgery2 The University of Texas Medical School at Houston Memorial Hermann Heart & Vascular Institute Introduction Blood transfusions worsen clinical outcomes in aortic surgery. Hemodilutional anemia increases organ ischemia risk. We show the lowest hematocrit (Hct) that reduces transfusion and prevents hemodilution associated complications. Methods We reviewed 399 cases of Ascending Aortic (Aneurysm or Type A dissection) repair with deep hypothermic circulatory arrest (DHCA). Demographics and surgical characteristics (except age) were similar between groups. Patient ages were 17-89 and are grouped by Hct <16%, <18%, 19%-20%, 21%-22%, > 23% at temperature < 20C, 20-28C, 28-32C, 3234C, 34-35C during CPB. Methods Databases were established by collecting medical information through patient medical records and 2010 ICD-9-CM Volume 1 Diagnosis Codes, including complications of surgical and medical care, not elsewhere classified 996-999 and diseases of the specific system or organ. The data analysis was by mean ( standard deviation) for continuous variables and by frequency (percentage) for qualitative variables. Two-sample t-test or Chi-Square test was used to compare groups with P-value of less than 0.05 considered significant. Results Changes in outcome were suggested at Hct <16% versus >16% at <20C during DHCA and also for Hct <18% versus>18% at temperature 20-28 C. Risk of ARF and postoperative tracheotomy increased with Hct < 16 (Table 2). Chance of discharge home improved with higher Hct at all temperatures (Table 3). Mortality decreased at Hct 21-22% at 20-34C and increased at Hct <16% during DHCA (Table 4). Results Results Conclusion Patient temperature affects oxygen demand, blood viscosity, oxygen carrying capacity and delivery. Hct value is a transfusion trigger and should change with body temperature during aortic surgery. Hct 21-22% appears favorable for CPB at 20-34C. Hct <16% during DHCA increases mortality. Hct <18% during rewarming (20-32C) increases postoperative ARF risk.