Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Behçet's disease wikipedia , lookup
Periodontal disease wikipedia , lookup
Globalization and disease wikipedia , lookup
Inflammation wikipedia , lookup
Germ theory of disease wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Inflammatory bowel disease wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Rheumatic fever wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
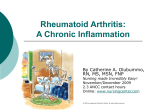
Recomendations for the medicamentous treatment of chronic inflammatory rheumatic disease pain Dušan Logar Dpt.of Rheumatology, University Clinical Centre, Ljubljana Rheumatoid arthritis RA is a chronic, inflammatory, systemic, autoimmune disease Mainly polyarticular disease Chronic inflammation in synovial membrane of affected joints The specific cause of RA is unknown, but the immune response is well characterised Pain in RA 71% adults who are taking methotrexate, biologics or both, continued to report pain 55% these individuals had to modify their daily household activities Arthritis Foundation Survey – 500 adult RA patients Pain in RA The extent of disability associated with chronic pain can vary from none to severe, and pain continue in the absence of tissue damage Interplay of various factors causing RA pain Cytokines Inflammatory mediators Synovial fluid Mechanical factors byochemical changes Neural-immune system interplay Glial cells Central sensitization Circadian rythm of various hormons Cells involved in articular inflammation Molecules involved in peripheral sensitization Tissue damage Inflammation Sympathetic terminals Sensitisizing cocteil BRADYKININE PROSTAGLANDINES CYTOKINES NA LEUCOTRIENES NERVE GROWTH FACTORS Hydrogen ions HISTAMINE NEUROPEPTIDES Potassium ions PURINES PROTEASES Direct action on nociceptors Sensitization of primary aferent neurons Transduction sensitivity IL-1β and TNF-α: Proinflammatory Cytokines in the Rheumatoid Joint High endothelial venule Bone Osteoblasts Synovial membrane O steoclasts Cartilage IL-8 PGE2 IL-6 Capsule TNF- a IL-1 Neutrophils Synovial space C hondrocytes Pannus Osteoblasts Osteoclasts Bone PGE2 = prostaglandin-E2 Dinarello C, Moldawer L. Proinflammatory and Anti-inflammatory Cytokines in Rheumatoid Arthritis: A Primer for Clinicians. 3rd ed. Thousand Oaks, Ca, USA: Amgen Inc.; 2001. Interplay of various factors causing RA pain Cytokines Inflammatory mediators Synovial fluid Mechanical factors byochemical changes Neural-immune system interplay Glial cells Central sensitization Circadian rythm of various hormons Interplay of various factors causing RA pain Cytokines Inflammatory mediators Synovial fluid Mechanical factors byochemical changes Neural-immune system interplay Glial cells Central sensitization Circadian rythm of various hormons Inflammmatory rheumatic disease pain Mast cell ARTHRITIS Macrophage Neutrophil granulocyte PHENOTYPIC SWITCH PERIPHERAL SENSITIZATION CENTRAL SENSITIZATION Zdravljenje bolečine pri revmatoidnem artritisu Treatment of chronic inflammatory rheumatic disease pain PARACETAMOL AND/OR NSAR, PARACETAMOL/TRAMADOL, OPIOIDS PAIN PATIENT EDUCATION, PHYSICAL THERAPY, ORTHOSES, BALNEOTHERAPY GLUCOCORTICOIDS DMARs, BIOLOGICS INFLAMMATION CORRECTIVE JOINT OPERATIONS DAMAGE OF JOINT STRUCTURES Pharmacological approaches NSAIDs DMARDs Biologics Intraarticular long acting steroids opioids Pharmacological approaches NSAIDs DMARDs Biologics Intraarticular long acting steroids opioids NSARDs Effectivness evaluation after 14 days Concommitant prescription of second NSARD is not allowed Risk of prescription NSARD with long t/2 to older patients Low dose therapy in children and old adults Do not to ignore contraindications: active ulcer disease ischaemic heart disease asthma, urticaria, angioedema advanced kidney disease Pharmacological approaches NSAIDs DMARDs Biologics Intraarticular long acting steroids opioids DMARDs Sulphasalasine Antimalarials Methotrexate Leflunomide Cyclosporine A Pharmacological approaches NSAIDs DMARDs Biologics Intraarticular long acting steroids opioids Biologics Infliximab Etanercept Adalimumab Rituximab Tociluzumab Pharmacological approaches NSAIDs DMARDs Biologics Intraarticular long acting steroids opioids Pharmacological approaches NSAIDs DMARDs Biologics Intraarticular long acting steroids opioids Opioids Treatment failure of therapy with NSARDs Contraindications for NSARDs Contraindications for corrective joint operation Patient long waiting on corrective joint operation Conclusions I 65 % patients with RA state pain as the most important symptom of the disease For 75 % of patients the still acceptable pain is graded with VAS between 0.5 and 2.0 Agressive treatment of RA with DMARDs and biologics decreases the need of analgetic use Future: targeted treatment with: Drugs that have influence on various ionic channels α-2 agonists Drugs that have influence on prostaglandine and opioid receptors in spinal cord Conclusions II Pain that is consistenly present in any rheumatic condition should be considered a specific disease entity, which should be actively managed in parallel with the rheumatic complaint Fitzcharles MA, Shir Y. New concept in rheumatic pain. Rheum Dis Clin North Am 2008;34: 267-83.