Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
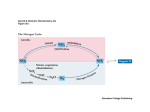
Pharmaconutrition: Selected Nutrients and Their Influence on Patient Outcomes The Canadian Clinical Practice Guidelines Daren K. Heyland, MD, FRCPC, MSc Queen’s University, Kingston, Ontario Updated July 2006 www.criticalcarenutrition.com Immunonutrition: Cocktail Approach? • Specific nutrients found to have effects on immune system, metabolism, and GI structure and function Arginine Glutamine Omega-3 fatty acids Nucleic acids others • Individual effect on clinical outcomes? Pathophysiology of Critical Illness endothelial dysfunction activation of coagulation/complement Insult • infection • trauma • I/R • hypoxemic/ hypotensive Role of GIT Arginine Activation of PMN’s elaboration of cytokines, NO, and other mediators generation of OFR (ROS + RNOS) mitochondrial dysfunction = oxidative stress cellular = energetic failure Key nutrient deficiencies (e.g. glutamine, selenium) organ = failure Death Elective Surgical Patient • cellular immune dysfunction – T-cell • decrease cytokine activation – IL-2, IFN Elective Surgical Patient arginase arginine expression of zeta chain Taheri Clin Cancer Res 2001 ;7:958 = 1.18 (0.88,1.58) Population Nutrients Which Nutrients? Which Patients? Elective Surgery Critically Ill General Septic Trauma Burns Acute Lung Injury Arginine Glutamine Omega 3 FFA Antioxidants Canadian Clinical Practice Guidelines JPEN 2003;27:355 www.criticalcarenutrition.com Underlying Rationale for Framework o No scientific rationale for combining nutrients together; need to consider them alone o Empirical evidence that the nutrients have different treatment effects across populations Which Nutrient for Which Population? Population Nutrients Elective Surgery Critically Ill General Septic Trauma Burns Acute Lung Injury Benefit No benefit Harm No benefit No benefit No benefit Glutamine Possible Benefit PN Beneficial (? receiving EN) … EN Possibly Beneficial EN Possibly Beneficial … Omega 3 FFA … … … … … Possible Benefit Antioxidants … Possible Benefit … … … … Arginine Canadian Clinical Practice Guidelines JPEN 2003;27:355 Arginine-supplemented diets? Underlying Pathophysiology Role of Nitric Oxide Mitaka Shock 2003;19: 305 Optimal NO-Balance cNOS - Microcirculation - Immune augmentation Harmful Arginine / NO availability cNOS + iNOS - Hemodynamic instability - Immune Suppression - Cytotoxicity - Organe dysfunction Suchner Brit J Nutrition Effect of Argininesupplemented diets on Mortality www.criticalcarenutrition.com Effect of Arginine-supplemented diets on Infectious complications www.criticalcarenutrition.com Effect of Arginine-supplemented diets in Critically Ill Patients • Possible mortality in septic pts. Crit Care Med 1995;23:436 Dent, Crit Care Med 2003 Bertolini Int Care Med 2003;29:834 • cost. • Lack of treatment effect. But what about ... Glutamine supplementation? Potential Beneficial Effects of Glutamine Enhanced insulin sensitivity Enhanced Heat Shock Protein Decreased Free Radical availability (Anti-inflammatory action) Inflammatory Cytokine Attenuation Glutamine Therapy Glutathione Synthesis Critical Illness Preservation of TCA Function Preserved Cellular EnergeticsATP content GLN GLN Pool pool Fuel for Enterocytes NF- B ? Maintenance of Reduced Translocation Intestinal Enteric Bacteria Mucosal Barrier or Endotoxins Nuclotide Synthesis Maintenance of Fuel for Anti-catabolic Lymphocyte Lymphocytes effect Function Preservation of Muscle mass Reduction of Infectious complications Effect of Glutamine: A Systematic Review of the Literature Infectious Complications www.criticalcarenutrition.com Effect of Glutamine: A Systematic Review of the Literature Mortality www.criticalcarenutrition.com Results of subgroup analysis Mortality EN PN Infection 0.80 (0.45-1.43) 0.83 (0.64-1.08) P=0.46 P=0.16 0.67 (0.48-0.92) 0.75(0.54-1.04) P=0.01 P=0.08 EN vs PN? Benefit of Parenteral Glutamine in Patients on EN? Fish Oil supplemented diets? Mechanisms of Action • Mediator formation depends on the phospholipid fatty acid content of arachidonic acid (AA) in inflammatory cell membranes • It is possible to modulate the content of AA in inflammatory cell membranes by changing lipid composition of the diet Mechanisms of Action GLA Arachidonic Acid Borage Oil EPA Fish Oil Cyclooxygenase Lipoxygenase Substitution of AA By EPA Resulting in: DGLA Substitution of AA By DGLA resulting in: PGE1 and Less Inflammatory Eicosanoids Decrease in Pro-Inflammatory Eicosanoids (LTB4, TXA2, PGE2) Less Inflammatory Eicosanoids (TXA3, PGE3, LTB5) Effect of Fish Oils/Borage Oils and antioxidants in Critically Ill with ALI 25 • RCT of 146 critically ill patients with ALI and BAL+ for WBCs 20 15 • Double-blinded; ITT • Experimental: Oxepa® Oxepa control 10 • Control: high fat diet 5 • Groups well matched at baseline 0 Vent Days ICU ICU Days Deaths P=0.03 P=0.02 P=0.17 Gadek Crit Care Med 1999;27:1409 Effect of Fish Oils/Borage Oils and antioxidants in Critically Ill with ALI • RCT of 100 critically ill patients with ALI • Single center • unblinded; not ITT 60 50 40 30 • Experimental: Oxepa® 20 • Control: high fat diet 10 • Oxepa associated with improved oxygenation and lung compliance Oxepa control 0 Vent Days ICU Days ICU Deaths Singer Crit Care Med 2006:34;1033 Effect of Fish Oils/Borage Oils and antioxidants in Critically Ill with ALI • RCT of 165 critically ill patients with ARDS secondary to sepsis • Double-blinded; not ITT • Experimental: Oxepa® • Control: high fat diet • Oxepa associated with: • improved oxygenation • More Vent free days • More ICU free days 50 45 40 35 30 25 20 15 10 5 0 Oxepa control Vent Days ICU ICU Days Deaths P=0.04 • Fewer new organ failures Pontes -Arruda Crit Care Med 2006:34;2345 Overall Effect on Mortality www.criticalcarenutrition.com Interpretation of Studies? • treatment effect of antioxidants? • treatment effect of borage oils? • comparison to standard enteral feeding products? How do you interpret the findings? Antioxidant-supplemented specialized diets? Rationale for Antioxidants Infection Inflammation Ischemia OFR CONSUMPTION OFR PRODUCTION Depletion of Antioxidant Enzymes OFR Scavengers Vitamins/Cofactors OFR production > OFR consumption = OXIDATIVE STRESS Impaired - organ function - immune function - mucosal barrier function Complications and Death Rationale for Antioxidants • Endogenous antioxidant defense mechanisms • Enzymes (superoxide dismutase, catalase, glutathione perioxidase, glutathione reductase including their cofactors Zn and Selenium) • Sulfhydryl group donors (glutathione) • Vitamins E, C, and B-carotene Rationale for Antioxidants 1. Pre-existing deficiencies - due to old age, smoking, malnutrition, chronic diseases 2. Increased requirements - high antioxidant consumption from high radical formation - high demands in hypermetabolism 3. Increased losses - skin exudate in burns, blood loss, dialysis, gastric aspirate, intestinal fistula 4. Reduced supply - posttraumatic, postoperative delay of adequate nutrition/ antioxidant supply - interruptions in nutrient supply because of clinical/ diagnostic procedures Effect of Combined Antioxidant Strategies in the Critically Ill Effect on Mortality Which Nutrient for Which Population? Population Nutrients Elective Surgery Critically Ill General Septic Trauma Burns Acute Lung Injury Benefit No benefit Harm No benefit No benefit No benefit Glutamine Possible Benefit PN Beneficial (? receiving EN) … EN Possibly Beneficial EN Possibly Beneficial … Omega 3 FFA … … … … … Possible Benefit Antioxidants … Possible Benefit … … … … Arginine Canadian Clinical Practice Guidelines JPEN 2003;27:355 ro a n Cri REducing Deaths from OXidative Stress: ials G i ad a l C ar e Tr t ic The REDOXS study up C an Factorial 2x2 design 1200 ICU patients Evidence of organ failure R glutamine R Concealed Stratified by site Shock placebo antioxidants placebo antioxidants R placebo Critical Care Nutrition Web Site www.criticalcarenutrition.com – web based clinical practice guidelines – summaries of evidence – online survey of current practice – benchmarking (other sites and the clinical practice guidelines) – tools (protocols, etc) – research related news