Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
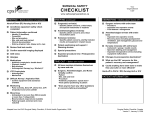
Daily Patient Goals – ICU/CCU Comments Action Items 7a – 7p Shift 7p – 7a Shift Number days line in________ Number days line in _______ Pain Management and Sedation - Neuro Cardiac/Volume Status Pulmonary / Ventilator Yes No Reintubation in the last 7 days? Yes No Readiness to Extubate? HOB > 30 degrees Sedation Scale Score? Vacation at 10:00 AM Oral Care PUD Prophylaxis DVT Prophylaxis GI / Nutrition / Bowel Regimen - Last BM ID, cultures, drug levels Can any catheters / tubes be removed? Central Line? Yes No Date Inserted ______/______/_______ Location of Central line____________________ Line placed ER CCU ____________ Skin care addressed? Were restraints used? Yes No Medication Changes (Can any be discontinued?) Test / procedures Scheduled labs, CXR: Can any be discontinued? Consultations - Who? When? Family communication – Updated? Social Issues? Emotional / Spiritual issues addressed? Code Status Addressed? Advance Directive in place? Mobilization / OOB Psych 1013 2013 Suicide Risk What needs to be done to discharge patient from ICU? Discharge Planning? Has this patient been readmitted to the ICU in the last 48 hours since ICU discharge? Yes No Comments: ____________________/____________________ Date ____/____/____ Nurses Signature Page 1 of 1 May 23, 2006 NOT PART OF MEDICAL RECORD RETURN TO INFECTION CONTROL PATIENT IDENTIFICATION