Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
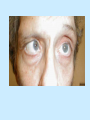
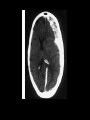
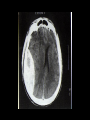
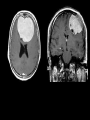
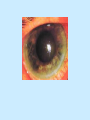
Emergency Nursing Course Neurological Emergencies Dr. Fu Tat Lee (李富達醫生) Princess Margaret Hospital (瑪嘉烈醫院) Outline Neurological assessment Stroke Seizure Acute generalized weakness Headache Neurological assessment What is it? Where is it? The Neurological Assessment • • • History should direct the neurological examination to the most relevant areas. Symptoms may occur before signs can be detected. In the absence of symptoms, any signs are less likely to be important. The Neurological Assessment • • • Look for asymmetrical abnormalities Tendon reflexes can be absent in health but may indicate an abnormality in the sensory or motor system An EXTENSOR PLANTAR REFLEX which is reproducible is never normal (except in infants) The Neurological Assessment A. Mental Status Glasgow Coma Scale B. Cranial nerves (1st - 12th) C.Upper & lower limbs - motor - sensory - coordination - reflexes eye opening motor response verbal response Decorticate posture Decerebrate posture Neurological Examination Cranial nerves (1) 1st (olfactory) nerve - anosmia (loss of smell) 2nd (optic) nerve - visual acuity - visual field Homonymous hemianopia Bitemporal hemianopia 3rd (Oculomotor), 4th (Trochlear) and 6th (Abducent) nerves - eye movements, upper eyelid & pupil size 5th (Trigeminal) nerve Motor: Masseter Sensory: ophthalmic, maxillary & mandibular divisions VII nerve (Facial nerve) Lower Motor Neuron lesion of VII nerve palsy Bell’s palsy - 1st described by Dr Charles Bell in 1882 - Lower Motor neuron lesion of 7th nerve - idiopathic etiology - Dx on i) no identifiable cause (viral/post viral Sx) ii) peripheral Symptoms Pain Tearing Drooling Hypersensitivity to sound Impairment of taste - DDx: Central 7th nerve palsy - sparing ipsilateral frontalis muscle Other causes of LMN lesion of VII nerve: Acoustic neuroma Parotid gland tumour Ramsey Hunt Syndrome: facial nerve palsy due to Herpes Zoster vesicles at the external auditory canal and ear. Bell’s palsy Treatment : - Prednisolone 60 mg daily for 5 days ? Acyclovir physiotherapy eyedrops and cover refer medical or ENT if fail to recover Prognosis : 80% recover completely within 3 months 8th (Acoustic) nerve - balance - deafness Weber & Rinnie Test to distinguish conductive deafness from sensory deafness Rinnie test Weber test 9th Glossopharyngeal nerve Muscles for swallowing 10th Vagus nerve Smooth muscles of GI & respiratory tract Pacemaker Muscles of heart, pharynx & Larynx gag reflex (sensory 9th) (motor 10th) 11th (accessory) nerve - sternomastoid & trapezius muscle 12th (hypoglossal) nerve - tongue Neurological Examination Upper & Lower limbs assessment Motor Posture, Muscle wasting, Fasciculation Muscle Tone: Hypertonic or Hypotonic Muscle power : Grading : 0 complete paralysis I flicker of contraction II movement is possible where gravity excluded III movement is possible against gravity but not if any further resistance is added IV movement is possible against gravity and some resistance V normal power Coordination Pastpointing, dysmetria, dysdiadochokinesia Romberg testing Gait Tendon Reflex Hyperreflexia or Hyporeflexia Plantar Reflex Upgoing or Downgoing Line of Stroke Normal Planter reflex Barbinski reflex Signs of Upper Motor Neurone Lesions Little muscles wasting unless from disuse Spasticity + Clonus Hyperreflexia Extensor Plantar response Signs of Lower Motor Neurone Lesions Wasting is prominent Fasciculation Hypotonia Hyporeflexia Normal or equivocal plantar reflex Sensation Temperature Light touch Temperature Pain Proprioception and vibration Dermatone Assessment of Brainstem function Brainstem reflex pupillary reactions corneal responses spontaneous eye movements oculocephalic responses (Doll’s eye reflex) oculo vesticular responses (Caloric test) respiratory patterns Stroke Stroke Stroke is a syndrome of rapidly developing clinical symptoms and signs of focal or global disturbances of cerebral functions due to non-traumatic vascular causes, with symptoms lasting more than 24 hours. Not a cerebrovascular “accident” but a consequence of cerebrovascular disease Stroke is preventable Modifiable risk factors History of stroke or TIA Hypertension Cardiac diseases Atrial fibrillation DM Internal carotid artery stenosis Smoking Alcohol abuse Hypercholesterolemia Obesity Lack of exercise Haematological diseases, coagulopathies Major types of stroke Ischaemic (70%) Intracerebral haemorrhage (25%) Cortical Subcortical Posterior circulation Lacunar infarction Supratentorial Infratentorial Both Subarachnoid haemorrhage (5%) Mortality & Morbidity Mortality at 1 month Mortality at 1 year Morbidity in survivors SAH 50% Intracerebral haemorrhage 40% 50% Cortical infarct 20% 35% Poor <2% Mild Lacunar infarct Severe Circle of Willis Principles of management Assess vital signs Confirm the diagnosis Differentiate ischaemic from haemorrhagic stroke Look out for clues for aetiology Screen for early complications Specific management of Ischaemic Stroke Stroke is an emergency Acute therapy is available for ischaemic stroke within 3 hours of onset. Tissue Plasminogen activator (TPA) 0.9mg/kg 10% as bolus and 90% infusion over 1 hour within 3 hours increases the proportion of patients with minimal or no disability by 13-16% 6% risk of transforming infarction into symptomatic haemorrhagic Antiplatelet therapy Low dose Aspirin (160 to 300mg daily) within 48 hours of onset prevents 11 recurrent ischaemic strokes or deaths at the expense of 2 extra cases of haemorrhagic transformation per thousand patients treated. ?? Glycoprotein IIb/IIIa inhibitor Anticoagulation Spontaneous haemorrhagic transformation of infarction commonly occurs within 2-4 days Clinical trials not support indiscriminate use of anticoagulation Neurosurgery Not needed in most cases Obstructive hydrocephalus Cerebellar haematoma or infarct Large superficial or lobar haematoma Markedly raised ICP Seizure Seizure - Primary epilepsy, idiopathic, onset before 20 - Secondary epilepsy, symptomatic, by parenchymal abnormality e.g. tumor, AVM, aneurysm, contusion/hematoma Different types of seizure - generalized/grand mal : witnessed LOC with generalized activities - minor/petit mal (absence) : prolonged unresponsive staring without LOC, + focal muscular activity - focal : repetitive motor activity without LOC - temporal lobe : hallucinations (visual, auditory, and olfactory), memory loss, and/or bizarre behavior which may progress to focal-generalized motor activity - Todd’s paralysis - focal weakness/paralysis after seizure lasting up to several days - febrile convulsion : 3 months to 5 years, rapidly rising fever Clinical evaluation ABCs examine for trauma including head/facial abrasions, contusions, lacerations, tongue, buccal lacerations Is patient seizing? Is patient awake? Look for eye deviation and focal/generalized tonic/clonic H’stix Treat reversible causes H3O H ypotension due to hypovolemia, arrhythmia H ypoxia H ypoglycemia O verdose & others (Electrolyte disturbance,Intracranial SOL, CVA, Infection) mnemonics of “ A E I O U” “T I PS” A Alcohol withdrawal T Temperature, Trauma E Epilepsy I Infection I Insulin P Psychogenic O Overdose & S drug withdrawal U Uraemia & Metabolic SOL, Shock Status epileticus Traditional definition: 30 minutes of continuous seizure activity or a series of seizures without return to full consciousness between the seizures. (D) Treatment support airway, IV, O2 and monitor treat reversible causes 1st line - Diazepam 0.25mg/kg IV or 0.5mg/kg PR - Lorazepam 0.1mg/kg iv - Midazolam 0.1 mg - 0.3 mg/Kg IVI or 0.2mg/kg IMI 2nd line - Phenytoin 18 mg/Kg IV load at 50mg/min with cardiac monitoring 3rd line - Consider phenobarbitone (200mg=1ml=1 Ampule) imi, generalized anaesthesia Discharge? Breakthrough seizure No underlying cause No head or other serious injury Good drug compliance No recent change on medication Escort by an responsible adult Acute generalized weakness Spinal cord compression Neuropathies Guillain-Barre syndrome Metallic poisons (lead & arsenic) Vitamin deficiencies (B12) Systemic diseases (DM, Renal failure) Drugs Acute generalized weakness Motor end plate Myasthenia gravis Botulism Eatom-Lambert syndrome Myopathies Acute periodic paralysis (Hyper, hypo or normokalemia) Alcoholic myopathy Polymyositis Drug (steroid) Guillain Barre Syndrome(GBS) George Charles Guillain Jean Alexandre Barre Guillain Barre Syndrome Pathology : An autoimmune disease causing acute demyelinating inflammatory polyradiculopathy GBS usually follow acute febrile illness, URTI, (days/weeks) typical pattern : symmetrical ascending flaccid motor paralysis, commonly with some sensory Symptoms (tingling sensation) Impaired breathing, BP and Heart rate BEWARE ! A&E patient with lower extremity weakness and loss of lower extremity reflexes Investigations & treatment Investigation Nerve conduction test CSF: high protein Management (mainly supportive) ICU care Ventilatory & circulatory support Plasmaparesis High dose Ig Psychological support GBS 90% weakest at the 3rd week Most patients recover What is the physical sign illustrated? Myasthenia Gravis - autoimmune disease - antibodies against acetylcholine receptors at the neuromuscular junction of striated muscle - Myasthenia Gravis bimodal distribution in age and gender, 2nd/3rd decade female; 6th/7th decade male - associated with thymic hyperplasia/thymoma - - complaints of muscle weakness, worsened by prolonged activity and improved with rest most common begin with ocular ptosis, diplopia and blurred vision - Respiratory failure - Confirm by bedside Tensilon test (Endrophonium) Headache Headache Tension headache Migraine Cluster headache Subarachnoid hemorrhage Hypertension (DBP >130mmHg) Meningitis Space occupying lesion Sinusitis Acute Glaucoma Postconcussion Temporal arteritis Trigeminal neuralgia Possible causes Intracranial Hemorrhage SAH, Subdural, Intracerebral Tumour Meningitis Vessel Migraine, Hypertension Extracranial Vessel Temporal arteritis Nerve Trigeminal neuralgia Muscle Tension Referred pain Acute glaucoma, Sinusitis Meningitis Meningitis Viral Bacterial Pneumococcus Meningococcus Haemophilus Influenzae Type B Kernig’s sign Brudzinski’s sign Temporal arteritis Trigeminal Neuralgia Watch out !!!! The first or the worst headache of patient’s life, especially the onset is acute and associated with neurology Progressively gets worse over days or weeks and subacute in onset Associated with fever, nausea and vomit Associated with neck stiffness, focal neurology, papilloedema, and changes in conscious level and cognition No obvious identifiable cause