Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Keratoconus wikipedia , lookup
Corrective lens wikipedia , lookup
Fundus photography wikipedia , lookup
Blast-related ocular trauma wikipedia , lookup
Contact lens wikipedia , lookup
Photoreceptor cell wikipedia , lookup
Idiopathic intracranial hypertension wikipedia , lookup
Dry eye syndrome wikipedia , lookup
Vision therapy wikipedia , lookup
Retinal waves wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
Eyeglass prescription wikipedia , lookup
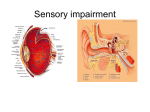
Visual impairment wikipedia , lookup
Retinitis pigmentosa wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
The Aging Eye January 5, 2004 Dorothy D. Sherwood, M.D. Cataracts • Cataracts are the leading cause of blindness world wide. • Cataract surgery is the most frequently performed surgical procedure in the US with 1.5 million operations annually • 50% of those over 65 develop vision impairing cataracts. Cataracts • Definition and Symptoms of Cataracts. – Clouding of the lens which prevents light from passing through properly to the retina – Types -3 Cataracts • Nuclear Cataracts – Most common age-related cataract • Substantial genetic component • Age, female sex, smoking are risk factors • More common in white • Cortical – Related to sun exposure – More common in blacks • Posterior Subcapsular – steroids Cataracts • Symptoms: – Cloudy vision, glare, halos, decreased night vision, faded colors, double vision, need for brighter light when reading • Treatment – can neither be prevented or treated with medications – surgical only – Removal of lens and insertion of intraocular lens (permanent) Cataracts • Indications for surgery – When visual impairment interferes with ADL’s, driving, working, – Co-existing ocular conditions requiring removal for treatment such as macular degeneration, diabetic retinopathy, glaucoma • Peri-operative evaluation- none – 19000 cases – no improved outcome with preoperative evaluation, except MI within 3 months – No need to stop anticoagulants or ASA-Archives – April 28, 2003 – 163(8):901-908 Cataracts • Peri-operative complications – Hypertension – Arrhythmia – 31 complications per 1000 procedures Cataracts • Surgical Strategies – Dilate eye and wash with povidone-iodine solution – Small self-sealing corneal or scleral incision is made for phacoemulsification tip and IOL – Injection of viscous material into anterior chamber to maintain the stability of the eye – Open the capsule with continuous tear capsulotomy, inject saline, separate lens from capsule with phacoemulsification Cataracts • Phacoemulsification introduced by Kelman in 1967 – Ultrasound probe using piezoelectric crystals to convert electrical energy into mechanical energy • Irrigation and aspiration of the cataract. The posterior capsule is kept intact. • Anesthesia is usually 1% lidocaine topical Cataracts • IOL – First implanted by Ridley in 1949 – Currently it is a small, foldable silicone or acrylic material injected into the capsule. – Monofocal or multifocal lens are available • Monofocal – distant vision only, near vision requires glasses • Multifocal – both – however, halos and loss of clarity are down side Cataracts • Postoperative Care – Topical eye drops • Antibiotics – gatifloxacin or moxifloxacin • Steroids for inflammation –prenisolone acetate 1% • NSAI drops – ketorolac tromethamine0.5% to prevent inflammation in the retinal • Examined one day, one week, two weeks, 1 months and 3 months post op – glasses can be prescribed in 2 weeks. Cataracts • Risk Benefits: – Bleeding, infection, posterior dislocation of lens material- intraoperative – Post operative -High-level of pressure in the eye, corneal swelling, retinal inflammation, dislocation of the IOL, retinal detachment, infection – Posterior capsule opacifications (PCO) – migration of lens remnants to the visual axis of the capsule – less common with improved technique – treat with laser Cataracts • Future – – Laser, ultrasound – less heat generated, – Pulse phacoemulsification – less heat – less chance for wound burn Cataracts • Take home – Most common cause of blindness worldwide, affecting 50% of the over 65 population – Clouding of the lens which impairs light travel to the retina. – Age, female sex, smoking, white – nuclear – Black, sun exposure – cortical – Steroids – subcapsular – MI 3 months prior is only risk factor- no preop evaluation needed. – Post op meds: gatifloxacin or moxifloxacin, prenisolone acetate 1%, and ketorolac tromethamine0.5%) Glaucoma • The triad of increased intraocular pressure, degeneration of the optic nerve head, restricted visual field – open angle glaucoma • Visual impairment in 0.7% of those over 60, 4% of those over 90 • IOP greater than 17.5 mmHg is associated with a persistent loss of vision and underscores the need to aggressively treat intraocular pressure Glaucoma • Diagnosed before loss of vision by ophthalmoscopic examination of the optic nerve to detect cupping. – – – – Blacks Advanced age Family history Elevated intraocular pressure- Goldman’s tonometer is gold standard – but the Schiotz indentation tonometer is cheap and easy to use – normal pressure is 15 to 16 mmHg – those with pressures over 21 are considered to have ocular hypertension Glaucoma • Dynamics of aqueous humor: – Produced by ciliary body, circulates around lens, through pupil, and anterior chamber – Flows out through the trabecular meshwork into the venous system –here-in lies the problem Glaucoma • Treatment is started when there is optic disc cupping or even when there is just elevated pressure >21 (normal 15). • The remainder of this discussion on glaucoma will cover the drugs used to treat this problem Glaucoma • Pharmacopoeia – Topical inhibition of carbonic anhydrase – Agonism of the alpha-adrenoceptor – Safer beta-adrenoceptor antagonist – Prostaglandin Analogues – Enhancement of trabeuclar outflow and uveoscleral outflow Glaucoma • Carbonic Anhydrase Inhibitors-sulfonamides- 1 drop tid – Inhibition of carbonic anhydrase in the eye results in decreased fluid transport across the ciliary body resulting in decreased formation of aqueous humor – Dorsolamide (Trusopt), brinzolamide (Azopt)- as effective as timolol, additive to timolol, brinzolamide is less irritant as its pH is 7.5 vs 5.6 – Burning, stinging, bitter taste, 15% - allergic conjunctivitis Glaucoma • [beta]-Adrenoceptor Antagonist– Timolol – (Timoptic) – used since 1979lowers intraocular pressure – the method of action is unknown, but may be related to decrease in aqueous humor production – Contraindicated in asthma, severe COPD, bradycardia, third degree heart block, CHF – Betaxolol – (Betoptic or Kerlone)- may have decreased bronchoconstriction and causes increased retinal blood flow. Glaucoma • Combination therapy – Dorsolamide and timolol (Corsopt) – decreases pressure by 50% • [alpha]-Adrenoceptor Agonists – Stimulate presynaptic feedback inhibition of norepinephrine and reduce aqueous humor formation. – .125% clonidine tid equal to pilocarpine, the standard • Doses of .25% or .5% produced hypotension – Brimonidine-(Alphagan)- reduces AH production, but also increases uveoscleral outflow - .2% tid – as effective as timolol • Headache, dry mouth, fatigue, ocular discomfort Glaucoma • Prostaglandin Analogs; – Latanoprost (Xalatan) –approved in 1996 – more effective than timolol bid and is only dosed qd. Causes increased pigmentation, growth of eyelashes, conjuctival hyperemia – Enhance uveoscleral outflow – Other drugs in same class: • Unoprotatone(Rescula), travoprost (Travatan), bimatoprost (Lumigan) Glaucoma • Muscarinic agents – parasympathomimetic drugs have been used since 1870’s. – Contraction of the muscle of the ciliary body – pulls scleral spur, opens trabecular meshwork, and increases aqueous flow form the eye – These agents are anticholinesterases • Pilocarpine -.25% to 4% every 4 to 8 hours as needed • Cause miosis and cataracts • Ocusert- wafer placed under the lid once a week – less side effects. Glaucoma • Cannabinoids – 1971- smoking marijuana lowers intraocular pressure by 45% – No successful topical form and systemic causes too many side effects Glaucoma • Take home points – – – – – – – DX and TX early – Schiotz tonometer, cupping of disc. Risk: Age, black, family history Drugs: CAI – decrease AH – Dorsolamide Alpha agonist – decrease AH - Brimonidine Beta blocker – unknown- Timolol Prostaglandin analog- scleral-uveal –Lantaoprost Muscarininc- opens the trabecula - Pilocarpine Macular Degeneration • Most common cause of blindness in the Western World – 8 million people world wide. Macular Degeneration • Macula is 5.5 mm in diameter, fovea is at its center – located temporally from the optic disc. • Fovea is thinnest part of the retina – no blood vessels • Preponderance of cone cells – detailed central vision Macular Degeneration • The retina is functionally 2 layers – Rods and cones – connected to the optic nerve – Retinal pigment epithemlium and its basal lamina called Bruch’s membrane – maintains the integrity of the barrier between the choroid and the retina – The choroid is between the retinal and the sclera Macular Degeneration • Causes: – Risk factors : age, soft drusen, macular pigmentary change, chorioidal neovascularisation in the other eye, hypertension, smoking, family history – The retinal pigment epithelium becomes less efficient – results in accumulation of waste material called drusen. The retinal pigment cells degenerate and central vision is lost – This is dry type age related MD – slowly progressive – 5 to 10 years to blindness Macular Degeneration • Geographic pattern of retinal pigment epithelial atrophy Macular Degeneration • Disruption of Bruch’s membrane– Choroidal neovascularizationedema – disruption of visual function – wet type or exudative age related MD Macular Degeneration • Clinical features – Blurring of the central vision – Reduced vision, metamorphopsia • The lines on graph paper will appear wavy or distorted – Ophthalmoscopic examination – chorioretinal atrophy on dry or macular edema on wet type, associated with retinal hemorrhages and lipid exudate Macular Degeneration • Retinal and choroidal angiography – Intraretinal hemorrhage and edema of macula – Fluorescein angiogram with leakage – Indocyanine green angiogram – choroidal vasculature Macular Degeneration • Clinical Advances – Laser treatments for choroidal neovascularization – Radiation treatment may preserve near vision and contrast sensitivity – Prevention: High dose Zn and Vit A,C,E – Lutein and zeaxanthin carotenoids – potent nativeantioxidants found in high concentration in the macula – needs to be studied – Suppression of vascular endothelial growth factor or other antiangiogenic agents Macular Degeneration • Take Home Points – Risk – age, soft drusen, htn, smoking, family history – Retina – retinal pigmented epithelium and rods and cones – Dry – failure of the RPE to remove waste products – results in accumulation of stuffatrophy – Wet- neovascularization of the Choroid – breaks Burch’s membrane-edema The Aging Eye • References: – “Age related macular degeneration”; BMJ Volume 326(7387); March 1 2003; pp 485-488 – “Recent Advances and Future Frontiers in Treating Age-Related Cataracts”; JAMA volume 290(2); July 9, 2003; pp248-251 – “Drug Therapy-Medical Management of Glaucoma”; volume 339(18); October 29 1998; pp1298-1307 – “New Glaucoma Medications in the Geriatric Population: Efficacy and Safety”; JAGS volume 50(5) May 2002; pp 956-962