Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
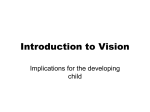
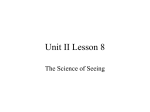
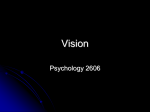
Grodno State Medical University VISUAL FUNCTIONS. CLINIC REFRACTION. Pavel Ch. Zavadski Assistant lecturer Of the Department of Ophthalmology VISUAL FUNCTIONS VISUAL ACUITY Visual acuity (VA) is the easiest to perform and most important test of visual function. Spatial visual acuity is the ability to distinguish separate elements of a target and identify it as a whole. It is quantified by the minimum angle of separation (subtended at the nodal point of the eye) between two objects that allow them to be perceived as separate. Early astronomers found two stars resolvable as separate if the distance between the stars subtend an angle of at least 1 minute of arc The standard test is the Snellen chart, consisting of rows of letters of decreasing size. Each row is numbered with the distance in meters at which each letter width subtends 1 minute of arc at the eye. Acuity is recorded as the reading distance (e.g. 6 meters) over the row number, of the smallest letter seen. If this is the 6 meter line, then VA is 6/6; if it is the 60 meter line then VA is 6/60. VISUAL ACUITY VISUAL ACUITY Peripheral vision is a part of vision that occurs outside the very center of gaze. There is a broad set of non-central points in the field of view that is included in the notion of peripheral vision. "Far peripheral" vision exists at the edges of the field of view, "mid-peripheral" vision exists in the middle of the field of view, and "nearperipheral", sometimes referred to as "para-central" vision, exists adjacent to the center of gaze. PERIFERAL VISION Each field can be represented as a series of contours or isopters, demonstrating the ability to resolve a target of given size and brightness. The field is not flat; towards the center the eye is able to detect much smaller objects than at the periphery. This produces a ‘hill of vision’ in which objects which are resolved in finest detail are at the peak of the hill (at the fovea). On the temporal side of the field is the blind spot. This corresponds to the optic nerve head where there is an absence of photoreceptors. The visual field may be tested in various ways. PERIFERAL VISION 1 2 3 4 5 6 PERIFERAL VISION These machines permit more accurate plotting of the visual field. They measure: •The kinetic visual field in which the patient indicates when he first sees a light of a specific size and brightness brought in from the periphery. This is rather like the moving pinhead of the confrontation test. •The static visual field in which the patient indicates when he first sees a stationary light of increasing brightness. These techniques are particularly useful in chronic ocular and neurological conditions to monitor changes in the visual field (e.g. in glaucoma). PERIFERAL VISION COLOUR VISION Colour vision testing is sometimes useful in the clinical evaluation of hereditary fundus dystrophies, where impairment may be present prior to the development of visual acuity and visual field changes. Colour vision is a function of three populations of retinal cones each with its specific sensitivity: blue (tritan) at 414-424nm, green (deuteran) 522-539 nm and red (protan) at 549-570nm. A normal person requires all these primary colours to match those within the spectrum. Any given cone pigment may be deficient (e.g. protanomaly - red weakness) or entirely absent (e.g. protanopia - red blindness). Trichromats possess all three types of cones (although not necessarily functioning perfectly) while absence of one or two types of cones renders an individual a dichromat or a monochromat respectively. Most individuals with congenital colour defects are anomalous trichromats and use abnormal proportions of the three primary colours to match those in the light spectrum. Those with red-green dellciency caused by abnormality of red-sensitive cones are protanomalous, those with abnormality of green-sensitive cones are deuteranomalous and those with blue-green dellciency caused by abnormality of blue-sensitive cones are tritanomalous. BINOCULAR VISION Binocular vision is the coordinated use of the two eyes in order to produce a single unified image in three dimensions. It is not present at birth. Three factors are required for its development: reasonably clear vision in both eyes, precise co-ordination between the eyes for all directions of gaze, ability of the visual areas of brain to promote fusion of the two slightly dissimilar objects. The three advantages of binocular vision are: 1) an enlarged field of vision with compensation of each blind spot, 2) an ability to appreciate depth with stereoscopic vision, 3) a combined binocular visual acuity is better than the uniocular visual acuity. COLOUR VISION Ishihara test is used mainly to screen for congenital protan and deuteran defects. It consists of a test plate followed by 16 plates each with a matrix of dots arranged to show a central shape or number which the subject is asked to identify. A colour deficient person will only be able to identify some of the figures. Inability to identify the test plate (provided visual acuity is sufficient) indicates malingering. Hardy-Rand-Rittler is similar to Ishihara but more sensitive since it can detect all three congenital defects. City University test consists of ten plates each containing a central colour and four peripheral colours. The subject selects one of the peripheral colours which most closely matches the central colour. DARK AND LIGHT ADAPTATION Dark adaptation is the phenomenon by which the visual system (pupil, retina and occipital cortex) adapts to decreased illumination. This test is particularly useful in the investigation of patients complaining of night-blindness (nyctalopia). The retina is exposed to an intense light for a time sufficient to bleach 15% or more of the rhodopsin in the retina. Following this normal rods are Insensitive to light and cones respond only to very bright stimuli. Subsequent recovery of light sensitivity can be monitored by placing the subject in the dark and periodically presenting spots of light of varying intensity in the visual field and asking the subject if they are perceived. Technique of Goldmann-Weekes adaptometry a. The subject is exposed to an intense light that bleaches the photoreceptors and then suddenly placed in the dark. b. The threshold at which the subject just perceives the light is plotted. c. The flashes are repeated at regular intervals: the sensitivity of the eye to light gradually increases. CLINICAL OPTICS Light can be defined as that part of the electro-magnetic spectrum to which the eye is sensitive. The visible part of the spectrum lies in the waveband of 390 nm to 760 nm. For the eye to generate accurate visual information light must be correctly focused on the retina. The focus must be adjustable to allow equally clear vision of near and distant objects. The cornea, or actually the air/tear interface is responsible for twothirds and the crystalline lens for one-third of the focusing power of the eye. These two refracting elements in the eye converge the rays of light because: 1) The cornea has a higher refractive index than air; the lens has a higher refractive index than the aqueous and vitreous humours that surround it. The velocity of light is reduced in a dense medium so that light is refracted towards the normal. When passing from the air to the cornea or aqueous to lens the rays therefore converge. 2) The refracting surfaces of the cornea and lens are spherically convex. CLINICAL OPTICS When parallel rays of light from a distant object are brought to focus on the retina with the eye at rest (i.e. not accommodating) the refractive state of the eye is known as emmetropia. Such an individual can see sharply in the distance. CLINICAL OPTICS In ametropia, parallel rays of light are not brought to a focus on the retina in an eye at rest. A change in refraction is required to achieve sharp vision. Ametropia may be divided into: 1) Myopia (short sightedness); the optical power of the eye is too high (usually due to an elongated globe) and parallel rays of light are brought to a focus in front of the retina 2) Hypermetropia (long sightedness); the optical power is too low (usually because the eye is too short) and parallel rays of light converge towards a point behind the retina. 3) Astigmatism; the optical power of the cornea in different planes is not equal. Parallel rays of light passing through these different planes are brought to different points of focus. Em M H Ast CLINICAL OPTICS All three types of ametropia can be corrected by wearing spectacle lenses. These diverge the rays in myopia, converge the rays in hypermetropia and correct for the non-spherical shape of the cornea in astigmatism It should be noted that in hypermetropia, accommodative effort will bring distant objects into focus by increasing the power of the lens. This will use up the accommodative reserve for near objects. Thank You For Your Attention