Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
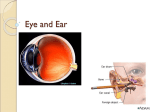
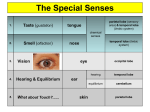
THE SENSORY SYSTEM GENERAL SENSES AND SPECIAL SENSES Sensory Receptor Dendrite of sensory neuron or specialized cell that monitors conditions in or around the body and sends information (sensation) to the CNS Special Senses—receptors localized in a specific organ General Senses—receptors are all over the body. Sensation and Perception Sensation- feeling or awareness of a stimuli Perception-the conscious interpretation of stimuli and involves the cerebral cortex Adaptation-with all receptors, long term stimulation leads to adaptation causing the perception of sensation to be less acute Sensation and Perception Mental state affects perception. Think of the perception of pain when we are sad and the perception of pain when we are happy, active and busy doing something. Sometimes will see or feel things that aren’t there (ex. Phantom limb pain; auras before epileptic seizures) General Senses 1. Temperature – separate receptors for hot and cold 2. Pressure-we can feel pressure even when skin is anesthetized. Receptors are found deep within the body as well as on the surface. 3. Touch-Preceptors are mostly in the dermis. Especially numerous on the fingertips, toes, lips, and the tip of your tongue General Senses 4.Pain- our most protective sense. The two types use the same receptors, but have different neural pathways. Two types: A. acute, sharp pain B. slow, chronic pain Analgesic- pain relieving drug 1. Non-narcotic analgesics (decrease inflammation) also known as NSAIDS example; acetaminophen (Tylenol, aspirin, ibuprofen 2. Narcotics- affect CNS and are habit forming- change the response to pain. Example; morphine and Demerol Pain Relievers Anesthetics- block pain sensation Endorphins- natural brain chemicals that inhibit pain centers in the brain Heat and cold application Relaxation and distraction techniques Pain Tolerance vs. Pain Threshold Everyone has about the same pain threshold ( point at which stimulation produces pain), but we have widely varying tolerance to pain Referred Pain Pain felt in a part of the body other than the place being stimulated. Examples; heart attack pain is often felt in the left arm rather than in the chest. Appendicitis is sometimes felt at the umbilicus rather than in the lower right quadrant 5.Propriception Sense of body position Cerebellum is the main coordinating center. Propriception monitors the position of joints and muscles involved in posture and balance Special Senses Vision Hearing Equilibrium Taste (gustation) Smell (olfaction) The Eye and Vision Eye is protected by: skull bones eyelids and eyelashes tears- lubricate and wash debris away conjunctiva- the membrane covering the visible portion of the eyeball and lining the eyelids 3 Layers (tunics/coats) of eye 1. Sclera- outer layer of tough connective tissue Contains the white of the eye (sclera) and cornea (clear). Gives shape to the eye. Muscles attached here help eye to move. Cornea- clear covering that bends light and is the first step in focusing 3 Layers (coats/tunics) of the eye 2.Choroid- middle layer, Made of Connective tissue with blood vessels. Contains the iris (the colored Part of eye- the muscle surrounding the pupil) 3 layers (coats/tunics) of the eye 3. Retina- inner layer. Contains visual receptors and neurons. Rods and cones are receptors for vision Contains many layers of nerve cells that transmit the impulses from the light rays to the optic nerve Rods- used for vision in dim or dark light and give a less sharp image Cones- used in bright light and are sensitive to color (red, green, blue) Retina continued Dark adaptation- going from dim to bright light or bright to dim light. It takes some time for vision to adjust (adapt) to a change in available light. Color blindness caused by the lack of one or more types of cones Retina Choroid Cornea Sclera Fovea Lens Aqueous humor Iris Optic Disc Vitreous humor Zonules Ciliary Body Refraction Bending of light—the path light follows through the eye 1. Cornea-part of sclera -transparent 2. Aqueous humor-fluid between the cornea and lens 3. Lens-clear-changes shape to focus light on the retina 4. Vitreous humor-gelatnous-helps give eyeball its shape Eye Muscles Intrinsic-within the eye Iris-colored part-the muscle controlling the size of the pupil (opening) which regulates the amount of light entering the eye Ciliary Body-surrounds the lens and changes the shape of the lens, helps to focus eyes Eye Muscles Accommodation-allows the eye to focus on near objects- the muscle contracts, the lens changes shape- gets thicker Accommodation decreases with aging Extrinsic- 6 muscles around the outside the eye. They move the eye Nerve Supply to Eye Optic Nerve (Cranial Nerve II)-takes info from the retina to the brain Optic disc-area of retina where the optic nerve attaches- no rods no cones -“blind spot” Fovea centralis-near optic disc-indented area on retina. Contains only cones. Area of sharpest vision 1 Branch of Trigeminal Nerve (Cranial Nerve V)takes sensation of pain, touch and temperature from the eye to the brain Accessory Structures of the Eye Conjunctiva-membrane that covers the inner surface of the eyelids and the front of the eye Lacrimal glandmakes tears Lacrimation=crying Lubricates the conjunctiva and outer part of eye, decrease friction, Prevents infection and nourishes the conjunctiva Opthalmologist Physician who deals with the diseases and disorders of the eye Surgical specialty Optician- makes glasses Optometrist- gives eye exam Eye Disorders Conjunctivitis-inflammation of the conjunctiva. “Pink Eye” very contagious. Cause: viruses, bacteria, irritants, allergies The ‘pink’ color is due to the dilation of blood vessels within the eye Stye- bacterial infection of a sebaceous gland along the eyelashes Eye Disorders Chlamydia trachomatis- chlamydia organism causes STD and inclusion conjuctivitis. Scars the conjunctiva and cornea and leads to blindness. In developing countries this is called ‘trachoma’ and is chronic. Treatment: antibiotics and good hygiene Ophthalmia neonatorum- eye infection newborns can get during birthcaused by gonorrhea, chlamydia or other STD Eye injuries Scratch or laceration of the corneavery common in contact lens wearers (don’t sleep in contacts or wear them multiple days in a row without removing and cleaning) Enucleation-removal of the eyeball Vision Defects Hyperopia- farsightedness. Eyeball is too short or shallow. Focal Point is behind the retina. See far objects well and near objects poorly Myopia- nearsightedness. Eyeball is too long. Focal point is in front of the retina Visual Defects Astigmatism –cornea and /or lens surface is irregular resulting in incorrect refraction and blurred vision Presbyopia –(old eye) lens loses its elasticity as people age resulting in farsightedness. The Lens does not accommodate well Visual Defects Treatment for all: corrective lens radial keratotomy (RK), photorefractive keratectomy (PRK)— laser surgery. RK and PRK involve making radial incisions into the cornea to correct refraction. Vision Defects (continued) Strabismus-eyes don’t work together. Extrinsic muscles are not coordinated. Convergent Eye wanders toward the median. Divergent strabismus- eye wanders to the side. If untreated, eventually the brain will not ‘see’ images from the affected eye. Treatment- eye patch, glasses, surgery Vision Defects Cataracts-lens becomes cloudy, Not transparent. Leads to a gradual loss of vision and blindness. Treatment- surgery to remove the old lens and implant artificial lens Vision Defects Glaucoma- excess pressure in aqueous humor. Most common in those over 40. Those who have this disorder will often see bluegreen halos around light. Increased pressure leads to blindness because of pressure on the optic nerve. Ophthalmologists and optometrists test pressure in the eye by bouncing a tiny blast of air off the surface of the eye. Treatment- drugs- eye drops Vision Defects Retinal Problems Diabetic Retinopathy- one of the leading causes of blindness in the U.S. Diabetes damages the retina because of changes in blood vessels Retinal detachment- retina separates from choroid. Cause: trauma or increased fluid between choroid and retina. Leads to blindness. Treatment: surgery using laser in spots to create scar tissue to connect retina to choroid Vision Defects Macular degenerationhardening and blockage of blood vessels in retina leading to blindness. New vessels form to replace damaged vessels- but the new vessels form on the retinal surface blocking light to the cones Vision Defects Floaters- spots in your vision Gray or black specks Vitreous humor becomes more liquid Microfibers within vitreous tend to clump together casting shadows on the retina The Ear and Hearing Organ of hearing and equilibrium The Ear 3 main parts External ear Middle ear Inner ear External Ear Pinna (auricle)- directs sound waves into ear External auditory canal-directs sound waves deeper into the ear Ceruminous glands produce cerum(ear wax) X = external meatus(opening)- entrance to the auditory canal Pinna auditory X External auditory canal Incus Semicircular canals Pinna Cochlea Malleus Eustacian or Pharyngotympanic or auditory tube Tympanic membrane vestibule stapes External Auditory Canal Middle Ear Tympanic Membrane-dividing point between external and middle ear. Vibrates with sound waves. Eustacian/auditory/ pharyngotympanic tubetube goes from the tympanic membrane to the pharynx (throat)equalizes pressure Middle Ear Auditory Ossicles- sends sound waves to the inner ear 3 tiny bones that amplify sound waves Malleus Incus Stapes Inner Ear Within temporal bone 3 parts: 1. Vestibule-connected to the oval window 2. Semi-circular canalsorgan of equilibrium 3. Cochlea-organ of hearing Ear Disorders Otitis Mediainflammation of the middle ear. Often caused by an upper respiratory infection. Pathogen goes up Eustacian tube- attracts white blood cells which leads to the ear filling with pus. If untreated, tympanic membrane can rupture leading to hearing loss. Treatment: antibiotics Ear Disorders Mastoiditis- pathogens from middle ear get into air pockets in the mastoid process of the temporal bone. Leads to severe earache, fever, swelling behind the ear. Untreated can spread to brain. Hearing Loss Conductive Deafness-problem with the passage of sound waves through the ear. Treatment: hearing aid, surgery to repair tympanic membrane or free auditory ossicles. Sometimes artificial ossicles are implanted Hearing loss Sensorineural Deafness- problem is in the cochlea or along the neural pathway. Treatment: few effective treatments. Cochlear implants Taste (gustation) Taste buds—clusters of taste receptors Gustatory cells live only about 10 days Receptors more responsive to bad tastes than good 4 Primary Tastes Sweet Salt Sour Bitter Gustation and olfaction work together. We are more aware of tastes when we can smell Taste Tasting ability decreases with age-elderly people sometimes find food to be tasteless which leads to poor eating habits. They can often taste sweet thing when other taste sensations have diminished. Children have lots of very active taste receptors, so they often don’t like spicy or strong flavored foods. Smell (olfaction) Olfactory receptors located in upper part of nasal cavity With inhalation , a small amount of air passes over the olfactory receptor. The chemicals in the air diffuse into the mucus of the nasal cavity and then stimulate the olfactory receptors At least 50 primary smells With age the # of receptor decreases, so smell becomes less acute