Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Attachment therapy wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Depersonalization disorder wikipedia , lookup
Cognitive behavioral therapy wikipedia , lookup
Effects of genocide on youth wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Asperger syndrome wikipedia , lookup
Memory disorder wikipedia , lookup
Diagnosis of Asperger syndrome wikipedia , lookup
Attachment disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
History of mental disorders wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Treatment of bipolar disorder wikipedia , lookup
Drug rehabilitation wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Externalizing disorders wikipedia , lookup
Veterans benefits for post-traumatic stress disorder in the United States wikipedia , lookup
Child psychopathology wikipedia , lookup
Combat stress reaction wikipedia , lookup
Posttraumatic stress disorder wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
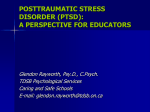
Complex PTSD Dr Felicity De Zuluetta Consultant Psychiatrist The Maudsley Hospital Dr Walter Busuttil Medical Director & Consultant Psychiatrist. Combat Stress [email protected] Aims of Workshop • • • • • • • • • • Part One Define Simple and Complex PTSD Multiple Traumatisation in Children and Adults Co-morbidity vs CPTSD Common presentations Differential Diagnosis What is the relationship between Complex PTSD, Dissociative Disorders, Borderline PD and Psychosis Part Two Management & Treatment Strategies Therapeutic Models of Intervention individual and Group Treatments Highlight outcomes of a 90-day inpatient programme for treatment of Complex PTSD Highlight new inpatient ward programme for Women Forensic Service Classification DSM-IV ICD-10 • Acute Stress Disorder • Acute PTSD • Chronic PTSD • Delayed PTSD • Acute Stress Reaction • PTSD • Enduring Personality Change Following Catastrophic Stress Relationship between: PTSReaction & PTSDisorder ASD & PTSD DSM & ICD ASD ----->Acute PTSD---->Chronic PTSD fluid state--------------------->fixed state 0___________________1________________________4________Months time in months PTSD CO-MORBIDITY: BIO/PSYCHO/SOCIAL • • • • • • • • • • • Depressive illness 50-75% Anxiety disorder 20 -40% Phobias 15 - 30% Panic disorder 5 -37% alcohol abuse / dependence 6 - 55% drug / abuse / dependence 25% Divorce Unemployment Accidents: RTA rates 49% higher in Vietnam vets than non-vets Suicide: 65% higher in combat veterans Symptom Overlap Differential diagnosis Aetiological Models of PTSD • Information Processing Model Prime model on which others are based on. • Psychosocial Model Support before, during and after exposure • Behavioural Model Triggers & stimulus generalisation • Cognitive Model Cognitive distortions (Ehlers & Clark) • Cognitive Appraisal Model Meaning of stressor & its effects on the future, -man-made vs acts of God. • Dual Representation Theory Situationally accessible memory versus verbally accessible memory • Biological Models Unproven & various FMRI studies • Attachment Theory Models Aetiology of PTSD Memory: Facts Feelings Sensations Stressor Triggers Arousal Re-experiencing Personality/ developmental stage/ social support Avoidance Depression/isolation/alcohol/illicit drugs/ guilt Biological Models for PTSD • Several neuro-transmitters involved. • Stimulation challenge tests – trigger exposure tests: Pre-frontal; Limbic; Peri-occipital • Functional MRI Scans: Amygdala, ‘fuse box’ blow-out. Proximity to narrative centres • In Borderline PD FMRI abnormalities are very similar indeed! What is Complex PTSD? Multiple vs Single Trauma • Multiple Exposure • Single Exposure • eg: CSA for five years • Road Traffic Accident • Falklands War • Lockerbie Clear up operation • eg Lockerbie Clearup operation Multiple Traumatisation Considerations: • Nature and Extent of Trauma Personal General • • • • • Age and Developmental Stage Reason / Cause / Ideology Support - Group vs Isolation Sustained - predictable / unpredictable Intermittent Traumatisation in Childhood • Age • Context - act of God / act of Man? • Multiple vs Single • Dose response? • Meaning • Developmental Stage • Brain development • Attachments • Open vs Secret • Individual vs Group • ABUSE: • Physical vs Sexual vs Emotional vs Mixed • Perpetrator / Power, Control, Choice. • Drug induced state • Systematic vs NonSystematic: Organized? Eg Pornographic ring? • Within an institution? DSM-IV Complex PTSD Working Party Study • Multiple traumatisation below the age of 26 years predicted development of Complex PTSD • Exposure to Multiple traumatisation after the age of 26 years did not predict Complex PTSD Simple & Complex PTSD Simple PTSD • Single Trauma • • • • • Complex PTSD Multiple Trauma Traumatised Under age of 14 / 26 Developmental stage Attachments Neuro-developmental stage Busuttil & Turner (UK Trauma Group 2000 discussion) • Postulation that adult victims of torture and incarceration (multiple trauma), more likely to develop Enduring Personality Change after Catastrophic Stress (ICD-10, 1992) and not straightforward PTSD and not Complex PTSD. • CPTSD is likely in Adult survivors of CSA, or exposure to severe multiple trauma under the age of 26 (DSM-IV working party, 1994). Complex PTSD DSM-IV Field Trials Adult survivors of CSA (van der Kolk et al, 1994) Alterations in 7 dimensions: • • • • • • • Affect & impulses: affect lability, anger / aggression, self mutilation, suicidal preoccupation. Attention & concentration: dissociation, amnesia, depersonalization Self-Perception: helplessness, guilt, shame. Perception of perpetrator: idealization of the perpetrator or feelings of vengeance. Relationships with others: isolation, mistrust, victim role, victimization of others Somatisation: GIT; CVS; Chronic pain, conversion etc. Systems of meaning: despair, hopelessness, major changes to previously well held beliefs Disorders of Extreme Stress Not Otherwise Specified (DESNOS) (Herman, 1992) • Defined in Adult Survivors of Childhood Sexual Abuse • DESNOS + PTSD = Complex PTSD (1995/6) 4th Edition Text Revision – DSMIV-TR, 2000 mentions: • An “associated constellation of symptoms may occur in association with an interpersonal stressor: • impaired affect modulation, • self–destructive and impulsive behaviour; • dissociative symptoms; • somatic complaints; • feelings of ineffectiveness; • shame, despair or hopelessness. And J Herman who first described the syndrome notes that they also • Feel permanently damaged; • Sustain a loss of previously sustained beliefs; • Show social withdrawal; • feel constantly threatened; • Show impaired relationships with others • Show a change from the individual’s previous personality characteristics”. Complex PTSD: A diagnostic framework- disturbance on three dimensions (Bloom, 1997) • Symptoms • Characterological / personality changes • Repetition of Harm Complex PTSD Disturbance on Three Dimensions (after Bloom 1999) • • Symptoms of : PTSD Somatic Affective Dissociation Characterological Changes of: Control: Traumatic Bonding Lens of Fear Relationships: Lens of extremity-attachment versus withdrawal Identity Changes: Self structures Internalized images of stress Malignant sense of self Fragmentation of the self • Repetition of Harm To the self - faulty boundary setting By others - battery, abuse Of others - become abusers Deliberate self harm Complex PTSD Dynamic Model PTSD Developmental / Attachments (Busuttil 2006 after Bloom 1998) Trapped in Time Memory Formation Automatic Repeated Trauma Conscious •Physical •Psychological •Social Learned Helplessness Adaptive Over-Coping (Dissociation) Maladaptive Coping Avoidance Dissociation Numbing Anger Learned Coping Poor Support Other LEs Aggression Addictions Depression Personality Recent Concepts Developmental Trauma Disorder in children & adolescents: • Exposure • Triggered dysregulation in response to trauma cues • Persistently altered attributions and expectations • Functional Impairment. Developmental Trauma Disorder: 1. Exposure to multiple or developmentally adverse interpersonal trauma eg abandonment, betrayal, physical or and sexual assaults threats to bodily integrity, coercive practices, emotional abuse, witnessing violence and death. Subjective experience – rage, betrayal, fear, resignation, defeat , shame. Developmental Trauma Disorder: 2 Triggered dysregulation in response to trauma cues Dysregulation (low or high) in presence of cues. Changes persist & do not return to baseline; not reduced in intensity by conscious awareness. 1. 2. 3. 4. 5. 6. Affective Somatic Behavioural Cognitive Relational Self-attribution Developmental Trauma Disorder: 3 Persistently altered attributions and expectations 1. 2. 3. 4. 5. 6. Negative self attribution Distrust of protective carer Loss of expectancy of protection by others Loss of trust in social agencies to protect Lack of recourse to social justice /retribution Inevitability of future victimisation Developmental Trauma Disorder: 4. Functional Impairment. 1. 2. 3. 4. 5. Educational Familial Peer Legal Vocational Domains of impairment children and Adolescents (Task Force) 1. 2. 3. 4. Attachment- uncertainty about the reliability & predictability of the world; boundary problems, distrust & suspiciousness; social isolation; interpersonal difficulties; difficultly attuning others emotional states; difficulty with perspective thinking; difficulty enlisting other people as allies. Biology – Sensorimotor developmental problems; hypersensitivity to physical contact; Analgesia; Problems with coordination, balance, body tone, difficulties localising skin contact; somatisation; increased medical problems across a vast span eg: pelvic pain; asthma; skin problems; autoimmune disorders; pseudo seizures. Affect Regulation - Difficulty with emotional self regulation; difficulty describing feelings and internal experience; problems knowing and describing internal states; difficulty communicating wishes and desires. Dissociation – Distinct alterations in states of consciousness; amnesia; depersonalisation and derealisation; two or more distinct states of consciousness, with impaired memory for state based events. Domains of impairment children and Adolescents (Task Force) contd 5 6 7 Behavioural Control – poor modulation of impulses; self destructive behaviour; aggression against others; pathological self soothing behaviours; sleep disturbances; eating disorders; substance abuse; excessive compliance; oppositional behaviour ; difficulty understanding and complying with rules; communication of traumatic past by reenactment in day to day behaviour or play (sexual, aggressive etc). Cognition – Difficulties in attention regulation and executive functioning; lack of sustained curiosity; problems with processing novel information; problems focussing on and completing tasks; problems with object constancy; difficulty planning and anticipating; problems understanding own contribution to what happens to them; learning difficulties; problems with language development; problems with orientation in time and space; acoustic and visual perceptual problems; impaired comprehension of complex visual spatial patterns. Self-Concept – Lack of a continuous predictable sense of self; poor sense of separateness; disturbances of body image; low self esteem; shame and guilt Clinical Presentation: Developmental Trauma Disorder Complex Trauma Task Force of the National Child Traumatic Stress Network • Arguments put forward by the Task Force to take up the DSM-IV CPTSD Working Party criteria – still relevant • Co-morbidity: studies of abused children include in order of frequency: 1. Separation anxiety disorder 2. Oppositional Defiant Disorder 3. Phobic Disorders 4. PTSD 5. ADHD • ??? Developmental Trauma Disorder is a useful diagnostic frame work CPTSD & Attachment Theory Limitations of the individual based anxiety model of PTSD • Most events qualifying for PTSD are not ‘beyond the range of usual human experience’. • None is so powerful that exposure typically leads to PTSD (Kessler et al,1999) • PTSD occurs less in well integrated communities than in fragmented ones. • Lack of social support is a major risk factor (NICE, 2005) eg Asylum seekers in the UK. The case for PTSD as a Sensitisation disorder of the Attachment system • Yehuda found that only victims of an RTA whose stress response led to a lower than normal release of cortisol developed PTSD. • She postulated that PTSD may reflect a ‘biologic sensitisation disorder rather than a post traumatic stress disorder’(1997). • Wang attributes this sensitisation to changes in the attachment system ie suppression of cortisol levels observed in insecurely attached children (1997). The effects of PTSD are transmitted down the generations • Low urinary cortisol levels in adult holocaust survivors with PTSD and in their adult offspring (Yehuda, 1997, 2002). • Israeli soldiers whose parents were Holocaust survivors had higher rates of PTSD than their counterparts. • Children of mothers who suffered from PTSD following 9/11 have lower levels of cortisol. • Low cortisol levels predispose to PTSD in later life. Transmission of vulnerability to PTSD • Attachment research shows a 75% correspondence between a mother’s attachment and that of her infant (Van Ijzendoorn et al. 1997) which can be reversed if mother’s behaviour is altered towards the child. • These findings show there is non-genetic transmission of the potential for PTSD and trauma related violence in PTSD afflicted communities. • This underlies the importance of prevention and socially based treatment interventions. Non genetic transgenerational transmission – 75% correspondence found between parents’ mental representation of attachment and the infant’s attachment security (Van Ijzendoorn, 1997). – Transmission of mother’s low levels of cortisol when suffering from PTSD to her infant (Yehuda et al., 2005) – Traumatised individuals who respond to stress with lower levels of cortisol than normal develop PTSD (Yehuda, 1997). important implications in terms of genetic evidence and anti-social behaviour transmission. Complex PTSD & Disorganised attachments • Patients with CPTSD can be understood as suffering from disorganised attachments with associated symptoms of PTSD which can be severe. Attunement with baby’ and Affect regulation • The caregiver responds to the infant’s signals by holding, caressing, smiling, feeding, stimulating or calming, giving meaning. • Her empathic interaction results in a child who can put himself in the mind of another and interact successfully Laying down the Templates for future interactions • These daily interactions provide the memories that the infants synthesize into internal “working models” (Bowlby). • These are internal representations or templates of how the attachment figure is likely to respond to the child’s attachment behaviour both now and in the future. The Brain substrate of Attachment Behaviour Involves • A great part of the right hemisphere. • the supra orbital area of the brain which is crucial in enabling us to empathise with others • Partly mediated by: endogenous Opiates and oxytocin (feel good factor) • dopamine (energised state of feeling) • serotonin (linked to levels of dominance in hierarchy). Representation of the Self & Secure attachments • Is closely intertwined with the internal representation of the attachment figure. • A securely attached child has a mental representation of the caregiver as responsive in times of trouble. • These children feel confident and are capable of empathy and forming good attachments. • A secure attachment is a primary defence against trauma induced psychopathology (Schore 1996). Reflective Functioning • The caregiver induces reflective functioning in the infant by: – giving meaning to the infant’s experiences, – sharing and predicting his/her behaviour This enables people to understand each other in terms of mental states, to interact successfully with others and is key to developing a sense of agency and continuity. (Fonagy and Target, 1997) Resilience factor • Empathic understanding from an outsider (teacher or relative) can compensate for effects of childhood abuse and protect against re-enactment and trauma. (Single external carer) Insecure attachments An insecure attachment is one in which the infant does not have a mental representation of a responsive caregiver in times of need. • These infants develop different strategies to gain proximity to their caregiver in order to survive. • There are 3 types of insecure attachment behaviour: – Group C: Anxious ambivalent type (12%) – Group A: Avoidant type (20-25%) – Group D: Disorganised (15%) Disorganised Attachment Behaviour • Their caregivers are frightening • Or they themselves are frightened because the child is already suffering, from PTSD. • This behaviour leaves the child in a state of fear without solution (Main & Hesse 1992; 1999). • Reflective functioning is severely impaired: the more impaired, the more disturbed is the individual. 1. Attachment and Dissociation • The infant’s psychobiological response to such states comprises 2 response patterns: – 1. ‘Fight-flight’ response mediated by Sympathetic system: • Blocks the reflective symbolic processing > traumatic experiences stored in sensory, somatic, behavioural and affective states. 2. Attachment and dissociation – If ‘fight-flight response is not possible, a parasympathetic dominant state takes over and the infant ‘freezes’ in order to conserve energy, – feign death and foster survival. – Vocalisation is inhibited. 3. Attachment and dissociation – In traumatic states of total helplessness, both responses are hyper-activated leading to an ‘inward flight’ or dissociative response. Eg: child looks down from the ceiling watching herself being abused. B. The resulting features of the Traumatic Attachment The Moral Defence: 1. Child cannot survive without a parent so child will take the blame for their suffering and thereby preserve their attachment and hope for a better parent in the future. 2. By blaming themselves, these children retain power and control as well as hope for a better parenting future (Fairbairn 1952). 3. This reinforces the identification with the the abusing parent like the Stockholm syndrome in adults. Origin of the triangle of abuse • Work with survivors of child abuse demonstrate that the abused child will usually be most most angry with the parent who let it happen ie the ‘Mother’. • This abusive triangle is internalised in the survivors ‘working models’ to be replayed as abuser, victim or observer depending on the context. Triangle of abuse •Abuser •V •A •C •Victim •C •A •V •Colluder 1. The Psycho-biology of child neglect & abuse Changes in the HPA axis in response to stress or separation 1. Reduced levels of cortisol and increased glucocorticoid receptors : increase PTSD vulnerability 2. Release of endogenous opiates : increase analgesia by cutting or self harm. 1. The Psycho-biology of child neglect & abuse A limited capacity to modulate: 1. Sympathetic dominant affects: terror, rage and elation, 2. Parasympathetic dominant affects: shame, disgust, and hopeless despair. Results in: Self-medication with drugs or alcohol Resort to violence to counter threat to Self ASSESSMENT The ASSESSMENT should be carried out: 1. In relation to the external system of social attachments 2. In terms of the internal system of working models and resulting cognitions and behaviour and levels of dissociation. 3. Need for a potential SECURE BASE to be established BEFORE starting treatment. Assessment of the external attachment system • Social network in community and in mental health services ie levels of family support, social support and involvement of Community Mental Health Teams. • Genogram to spot deaths in family and important information left out of interview. • Bubble chart of services and people involved with client to pre-empt problems due to ‘splitting’, failure of communication etc Assessment of the external attachment system (cont) Cultural issues need to be taken into account: – Eg: Bangladesh family – Respect for parents in many cultures in Africa, Middle East – Implications of rape in similar cultures Reinforcement & Maintaining Factors: Important in relation to patients involved in domestic violence or sexual abuse or when patient’s illness is systemically reinforced by the family. • Eg of assessment failure • Eg domestic violence treatment problematic Assessment of the Internal Attachment System • Through the assessment of the internal world of working models (object relations) and security of attachment: – Use of questions in Adult Attachment Interview: ie. when you were little whom did you go to when you were hurt or upset? Incoherence in time: use of present when talking of somebody who has died. Capacity for reflective functioning ie putting him or herself into mind of the other Assessing the disorganised or ‘traumatic attachment’ • Look for the main features: – a strong ‘moral defence’ – idealisation and splitting, – resistance to change > traumatic attachment bonds to caregiver. • Look for levels of dissociation: Use of Dissociation Evaluation Scale (DES) Implications of the phenomenon of dissociation The phenomenon of dissociation should no longer be ignored in our understanding of such phenomena as: – – – – – Inexplicable shifts in affect Discontinuities in train of thought. Changes in facial appearance, speech and mannerisms. Apparently inexplicable behaviour. Somatic dissociative phenomena. Differential Diagnosis Multiple Traumatisation • Complex PTSD • Psychotic Illnesses: Schizophrenia / Bip Aff Dis • Borderline Personality Disorder • Dissociative Disorders • Enduring Personality Change After Catastrophic Stress Complex Trauma Reactions What is the central Hub of CPTSD? Somatoform Symptoms PTSD Borderline PD Psychotic Symptoms Dissociative Symptoms Relationship between PTSD and Psychosis 1. Psychotic symptoms among patients with primary PTSD (PTSD symptoms that are psychotic). – high dose stressor; chronic disorder; multiple childhood trauma 2. PTSD in the context of dual diagnosis – e.g. comorbid drug induced psychosis, co-morbid schizophreniform functional disorder, co-morbid psychotic affective disorder. 3. Misdiagnosis – either misinterpretation of primary PTSD symptoms or of co-morbid symptoms or both (common??) Misdiagnosis – either misinterpretation of primary PTSD symptoms or of co-morbid symptoms or both (very very common!!) Phenomenology: Single event or Simple PTSD Re-experiencing Psychosis 1. Nightmares 2. Recurrent intrusive images, thoughts, perceptions 1. Was this screened for in history taking? 2. Perceptual hallucinations; thought disorder 3. Recurrent Feelings as if it were recurring (incl reliving – illusions, hallucinations, dissociative flashbacks incl those occurring on wakening) 3. Flashbacks can occur in any sensory modality and can be misinterpreted as psychotic hallucinations / delusions in any sensory modality 4. Psychol distress on exposure to reminders of trauma 4. ?behavioural disturbance? Disinhibition? 5. Physiological reactivity 5. ?agitation? Borderline Personality Disorder DSM-4 criteria • • • • • • • • • Frantic efforts to avoid real / imagined abandonment Intense unstable interpersonal relationships Identity disturbance Impulsivity - self damaging: driving, sexual, binge eating Suicidal gestures / self mutilation Affective instability Chronic feelings of emptiness Anger: intense / inappropriate / difficulty controlling Transient Paranoid Ideation / Dissociation (stress related) Distinguishing Features from ComplexPTSD (Gunderson, 1993) • Absence of core cluster features of PTSD in BPD • Fear of aloneness is a core feature of BPD, absent in PTSD Trauma History CPTSD & BPD CPTSD • + Extreme Multiple Childhood Trauma • + Attachment difficulties deprivation BPD • - Extreme Multiple Childhood Trauma • + Attachment difficulties deprivation Complex PTSD • • • Symptoms of : PTSD Somatic Affective Dissociation Characterological Changes of: Borderline Personality Disorder • • Symptoms of : Transient Paranoid Ideation Affective Dissociation Impulsivity Characterological Changes of: Control: Traumatic Bonding Lens of Fear Relationships: Lens of extremityattachment versus withdrawal Control: Traumatic Bonding Lens of Fear Relationships: Lens of extremity-attachment versus withdrawal Identity Changes: Self structures Internalized images of stress Malignant sense of self Fragmentation of the self Identity Changes: Self structures Internalized images of stress Malignant sense of self Fragmentation of the self Repetition of Harm To the self - faulty boundary setting By others - battery, abuse Of others - become abusers Deliberate self harm • Repetition of Harm To the self - faulty boundary setting By others - battery, abuse Of others - become abusers Deliberate self harm Dissociation and PTSD: easy practical classification • Primary: dissociation at time of trauma – peri-traumatic – • Secondary: dissociation as part of a flashback – re-enactments • Tertiary: ‘flight to safety’- ‘blanking it off’- Dissociative Disorders • • • • • Dissociative Amnesia Dissociative Fugue Dissociative Identity Disorder Depersonalization Syndrome Dissociative disorder not otherwise specified • NB: Dissociative symptoms also included in criteria for ASD; PTSD & Somatisation Disorder. An additional Dissociative Disorder diagnosis is not given if the dissociative symptoms occur exclusively within one of these disorders. Multiple Traumatisation in Adulthood KZ Syndrome Konzentrations Lager Syndrome: Concentration Camp Syndrome (Herman & Thygersen, 1953) Characterized by 12 severe chronic psychiatric and non-specific somatic symptoms comprising: • fatigue • impaired memory • dysphoria • emotional instability • sleep impairment • feelings of insufficiency • loss of initiative • nervousness • restlessness & irritability • vertigo • vegetative lability Concentration Camp Syndrome (Herman & Thygersen, 1953) Associated symptoms (Eitinger1961) Associated symptoms Friedman, 1949): • • • • • • • • • • • anxiety nightmares depression alcohol abuse reduced alcohol tolerance re-experiencing symptoms emotional numbing apathy survivor guilt psychosomatic symptoms anxiety hyperarousal Associated symptoms Chodoff, 1963 • Avoidance symptoms Aetiology of Concentration Camp Syndrome Organic vs Psychological / Psychiatric vs Combination of Both • Organic brain damage - from starvation, avitaminosis, head trauma and fevers such as “spotted fever” (Eitinger 1961, 64; Thygersen, 1970). • In POWs of WWII & Korean war, Weight loss of 35% or over correlates with high incidence of more severe biological and psychological insult and PTSD and depression more likely to be present (Sutker et al, 1990; Speed et al, 1989). Multiple Traumatisation in Adults Hostages and POWs (Busuttil, 1992) • Stress Disorders (incl ASD & PTSD): pre-captivity experiences; initial captivity experience; torture; solitary & group confinement • Depressive Disorders: torture, loss events, captivity experience itself • Cognitive Defect States: weight loss, vitamin deficiencies, CNS infections, head trauma • Psychotic States: isolation and confinement • Personality - Character Changes: captivity experience itself: coping style and locus of control • Physical Illness - Somatiform & Genuine Busuttil & Turner (UK Trauma Group 2000 discussion for DSM-V) • Postulation that victims of torture and incarceration develop Enduring Personality Change after Catastrophic Stress (ICD-10, 1992) and not straightforward PTSD and not Complex PTSD. • The latter is likely in Adult survivors of CSA, or exposure to severe multiple trauma under the age of 26 (DSM-IV working party, 1994). Enduring Personality Change after Catastrophic Stress (ICD-10, 1992) Prolonged exposure to life threat/s PTSD may precede the disorder features seen after exposure to threat: • a hostile mistrustful attitude towards the world • social withdrawal • feelings of emptiness or hopelessness • chronic feelings of being on edge or threatened • estrangement Part Two Management Issues (W.Busuttil) 1 Politics: NICE Treatment Guidelines 2005 • Deal with Simple PTSD only • Guidelines do NOT deal with Complex PTSD or Chronic PTSD. • Next instalment might deal with CPTSD and Chronic PTSD(in four years time) UK Trauma Group Statement on CPTSD (May 2008) • NICE states that PTSD develops following a stressful event or situation of an exceptionally threatening or catastrophic nature, and examples that are given include single events such as assaults or road traffic accidents. • For adults, we believe that this refers to “simple” PTSD, which commonly develops following a single traumatic event occurring in adulthood. The recommended treatment is brief, trauma-focused psychological therapy. • However, the guideline does not apply to situations involving complex trauma, for example where there is a history of multiple traumatic events, including previous childhood trauma and attachment disorder. UK Trauma Group (May 2008) • The NICE guidelines do not provide adequate guidance in relation to the assessment and treatment of Complex PTSD. • This results in lack of appropriate provision, resources and training to treat people with Complex PTSD, and ensuing limited access to effective treatment services. • We propose that a review of the literature on complex PTSD is urgently needed to refine the definition of complex PTSD, and provide more detailed guidance for good practice in the assessment and treatment of complex PTSD. • We advise that the multi-phasic treatment recommendations outlined above should be followed as best practice for the treatment of Complex PTSD as we currently understand it. UK Trauma Group (May 2008) • Literature on effective treatment for complex PTSD is limited, but what there is so far shows that multi-phasic and multi-modal treatment is indicated for children and adults (e.g. Luxenberg et al., 2001). • The literature recommends that the following three stages are included: 1. Establishing stabilisation and safety; 2. Psychological therapy, incorporating trauma-focused elements and some exposure to the trauma; 3. Rehabilitation. Treatment of Complex PTSD: Basic Principles (Herman 1992; Bloom 1999) • Stabilization & Safety • Working through of Traumatic material – disclosure – psychotherapy • Rehabilitation Treatment of PTSD: Basic Principles • • • • • Multimodal Assessment Stabilise – Enhance Coping , Medication Therapy Outpatient vs Inpatient Safety - supports Treatment Pitfalls: • • • • • • • Common maintaining factors Nature and duration of trauma Role in trauma Meaning of trauma Has trauma ended? Isolation - attachments Guilt - omission / commission Guilt - survivor • • • • • • Other Factors Co-morbidity - treat this first? Alcohol & Illicit Drugs Motivation Co-operation Compliance Therapeutic qualities of patient & therapist Treatment of PTSD: Medications Drugs used: Neurotransmitter • adrenergic • adrenergic & serotonergic • B-blockers, alpha-2-agonists • TCAs & MAOIs • antikindling drugs • • • • • dopamine system • neuroleptics • GABA benzodiazepine system • opioid system • alprazolam, benzodiazepines, clonazepam • serotonergic SSRIs, 5HT1a agonist; 5HT2antagonist SNRIs Carbamazepine, valproate Lithium • naltrexone Medications: Medication Indication • Antidepressant • PTSD & Depressive symptoms • Neuroleptic • Pseudo-hallucinations; Dissociation; Tranquilization • PTSD Symptoms & Mood stabilizing properties • Mood Stabilizer / Antiepileptic • Anti-impulse • Impulse control - self- harm / depression Safety & Stabilisation • • • • • • • Safe environment Skills training, eg: DBT Interactive Psychoeducation Ward Structure and Programme Reward good behaviour Little attention to DSH Medications: used to stabilize patient in order to allow psychotherapy to be conducted primarily. After psychotherapy is finished, attempt should be made to reduce medications. Specific treatment models Engagement, Stabilisation / Skills trg: • Art Therapy • DBT • Body / sensori motor / energy therapies • Psychodynamic / analytical Psychotherapy Trauma Focussed • EMDR • CBT • Schema Focussed Therapy Sensori-Motor Interventions • Emerging • Overlap with other approaches • Body symptoms, automatic responses, posture, body language etc • Paying attention to the body, • Uses body rather than cognition or emotion as primary entry point to access trauma TF-CBT • Psycho-education • Disclosure / Exposure / Working Through of Traumatic Material • Cognitive restructuring • Problem solving • Use of behavioural techniques for example anxiety management TF-CBT Approaches • Exposure: The therapist helps confrontation of the traumatic memories (written, verbal, narrative). Detailed recounting of the traumatic experience – repetition. In vivo repeated exposure to avoided and fearevoking situations that are now safe but that are associated with the traumatic experience. CBT Approaches • Cognitive Therapy Focus on the identification and modification of misinterpretations that lead PTSD sufferer to overestimate current threat (fear) Modification of beliefs related to other aspects of the experience and how the individual interprets their behaviour during the trauma (eg: issues concerning shame and guilt). Other - CBT Approaches • • • • • • • Stress Management Relaxation Trg Breathing re-Trg Positive thinking and Self-talk Assertiveness Training Thought Stopping Stress Inoculation Trg EMDR (Eye movement Desensitisation and Reprocessing) • • • • • • Therapeutic rapport Imagery / envisioning of traumatic scenes Focus on sensations of anxiety Cognitive restructuring Saccadic movements of Eyes Extinguishing of the memory • Other methods - eg Counting Method • Need training - Criticisms EMDR • Standardised, trauma focussed procedure with several elements, always involving the use of bilateral physical stimulation (eye movements, taps, tones), thought to stimulate the individual’s own information processing in order to help integrate the targeted event as an adaptive contextualised memory • Requires individual to focus on a traumatic memory and generate a statement summarising thoughts of the trauma eg I should have done ‘X’ • Patient is instructed to visualise traumatic scene , briefly rehearse the belief statement that best summarised their memories, concentrate on their associated physical sensations, and visually track the therapist’s index finger. • Finger moved rapidly /rhythmically back & forth across line of vision – extreme l eft to right distance of 30-35cm from face at a rate of two back and forth movements per second. • This is repeated 12 – 24 times after which patient asked to blank picture out and take a deep breath • At the same time patient asked to focus on bodily experience associated with image as well as on an incompatible belief statement (eg I did my best; It is all in the past). • Therapist records subjective unit of distress (SUD), if has not decreased checks that scene has not changed • If has changed peocedure is repeated with new scene before returning to old one (Shapiro, 1989) Specific Treatment Models Children and Adolescents Development Trauma Disorder • • • • • • • ARC Model: Attachment; Self Regulation and Competency Model (Kinniburgh et al, 2005) Outpatient based Grounded in theory and empirical knowledge Includes systematic family intervention Recognises the core effects of trauma exposure on attachment, self regulation and development competencies. Emphasises the importance of understanding and intervening with the child in own context Philosophy that systemic change leads to effective and sustainable outcomes Not a manualised treatment protocol – a guideline framework tailor made for the individual. ARC Model Systemic ; Familial; Individual Attachment Training Individually Tailored approaches Primary components: Routines rituals Caregiver affect management attunement praise and reinforcement Regulation Competency Training Training Individually tailored approach Primary components Affect Training Identification Safe expression modulation Individually Tailored approaches Adjunctive activities eg sports Arts Community programming Primary Components Mastery Building connections Enhancing strengths Promote self efficacy Treating CPTSD in Adults Models: • DBT followed by TF Work • Self- Trauma Model & Trauma Focussed work • Psychodynamic therapy followed by Trauma Focussed work • Schema Focussed Therapy • Structured Group Therapy Programmes Dialectic Behaviour Therapy • DBT : developed by Marsha Linehan • A form of CBT developed to address Borderline PD and associated problems • Especially suicidal and self harming behaviours Dialectic Behaviour Therapy For: Life threatening Behaviours • Suicidal behaviours – attempts and ideation • Aggression & Violence Problems associated with Quality of Life • • • • • Alcohol & drug abuse Disordered eating Emotional and mood disturbance Poor impulse control Interpersonal problems Dialectic Behaviour Therapy: Programme • One year long • Once weekly individual therapy sessions with DBT trained therapist (1 hour long) • Once weekly group skills training session 1-2 hours long • Once weekly Consultation Meeting between therapists Functions and Modes of DBT: Functions • • • • Learning new skills Increasing Motivation Generalisation to the environment Therapists’ support and assuring motivation Modes • • • • Skills training groups Individual therapy (Ward based milieu) Team consultation DBT: Hierarchy of Targets: Pre-therapy: • Orientation • Commitment Stability, Connection & Safety Decrease in: • Suicidal / self harming behaviours • Therapy Interfering behaviours • Quality of life Interfering behaviours Increase in • Behavioural skills DBT: Skills Modules: • Mindfulness: control the mind: wise mind integration of emotion and reason, balanced knowing, intuition, peace of mind. • Emotional Regulation: objectives effectiveness; relationship effectiveness; self respect effectiveness. • Interpersonal Effectiveness: identifying factors that interfere with interpersonal effectiveness: lack of skill; worry thoughts and myths; excessive emotions; indecisive about priorities; environmental restraints. • Distress Tolerance: Crisis survival skills; Gudelines for accepting reality Skills Training Increase Decrease Mindfulness Identity confusion Emptiness Cognitive Dysregulation Interpersonal Skills Interpersonal Chaos Fears of abandonment Emotional Regulation Skills Affect lability Excessive Anger Distress Tolerance Impulsive Behaviour Suicidal Threat Automultilation DBT Individual Therapy • • • • • Structures Behavioural Cognitive -Behavioural Teaching guiding modelling testing out Strategies to over come invalidating environment • Weekly Home work; monitoring diary Skills Training Structure of the training • • • • • • Two times sequence over one year Every module comprises six weeks Every session takes 2.5 hours incl breaks Trainer and Co –trainer Videotaping Telephone consultation only possible to repair contact or to inform about home work • No psychodynamic group therapy • The trainers are members of the (staff) consultation team The Self Trauma Model (Briere) • Integrated Approach • CBT & Relational • Take symptoms beyond PTSD into account – address them • Titrated exposure to traumatic material • Affect regulation training • Trigger identification • Mindfulness as cognitive and affect regulation Therapeutic relationship emphased • Attendance / compliance • Context for support / validation / safety • Activates relations schema which then can be addressed. • Counter conditions relational trauma memories • • • • • • • Affect regulation training Dealing with acute intrusions – grounding Breathing training Identifying and discriminating emotions Countering intrusive and exacerbating intrusions Development of equimany through mindfulness Repeated exposure and processing as affect regulation training Affect Regulation – the content is not as important as the skill itself Mindfulness as a cognitive intervention Self observation: • Moment by moment of awareness of internal experience without judgement • Learning to let go of thoughts & feelings without avoidance or suppression • Focus on monkey mind / apes movies Especially childhood memories Thoughts are not perceptions, perceptions do not necessarily reflect reality Mediation of abuse related cognitive distortions and associated emotions Central Components of Trauma Processing • Exposure • Activation – triggers associated thoughts feelings – reliving • Disparity – although in activated state – now able to talk to therapist in safe environment: fear is therefore not reinforced : negative state generated in a safe environment • Central focus is on awareness: reliving trauma memories, thoughts, feelings – yet maintain current awareness experience ( safe): able to perceive the disparity memory of bad experience activated but need to be present in the here and now co awareness remember it as past aware that this is present. • Working with traumatic memory – activate the specifics of the memory cue her memory by asking question about what happened – helps processing Therapeutic Window Titrated exposure • Balance between therapeutic challenge and overwhelming internal experience • Maximal possible exposure & reactivation within the limits of affect regulation activity Overshooting vs undershooting the window Identity Development • Exploration of self in the context of the therapeutic relationship • Self knowledge • Self directedness • Value of not leaving open-ended questions • Avoiding over use of interpretations What is schema therapy? (Dr Julie Parker) • Schema therapy developed as a result of limitations of CBT in dealing with problems presented by people with underlying personality disorder • Many patients who have poor CBT outcome with Axis 1 disorder have an underlying PD e.g. a male patient undergoes CBT for OCD, when his symptoms are treated he has to face a life almost devoid of social contact. This lifestyle is a result of such an acute sensitivity to slights/rejections that he has avoided most social contact since childhood. He must grapple with the ‘defectiveness schema’ that underlies this problem if he is to have a rewarding life. Problems with CBT & PD issues Traditional CBT assumes that patients: • will comply with necessary aspects of therapy • are motivated & able to work with the therapist to reduce symptoms, build skills etc – for PD patients some primary symptoms are schema coping • can access thoughts & feelings –many PD patients engage in cognitive & affective avoidance • can change problem cognitions/behaviours through logical analysis, experimentation – PD patients are often psychologically rigid • can collaborate with the therapist – many PD patients have had disturbed relationships throughout their lives and have difficulty forming trusting relationships • PD patients ‘symptoms’ are ego-syntonic – they feel right & like a part of them How does schema therapy differ from CBT? Expands on CBT by drawing on techniques from other schools of therapy Greater emphasis on • Exploring childhood & adolescent origins of psychological problems • On emotive techniques • On the therapist-patient relationship • On maladaptive coping styles • Often undertaken in conjunction with other therapies & meds • For treating characterological problems not acute symptoms Psychodynamic / TF-CBT Models • Contrast with Briere’s Model: • De Zulueta’s (2002) model of intervention at the Maudsley Trauma Therapy Unit uses individual psychodynamic psychotherapies to deal with interpersonal and attachment issues before using Trauma-Focussed CognitiveBehavioural Therapy (TF-CBT). Dealing with dissociation • Its management requires a good attachment relation in therapy and techniques to reduce its frequency and intensity. • Aim when dealing with trauma is to maintain ‘one foot in the past and one in the present’. • Issues of shame • Grounding techniques for dissociation. Importance of therapist’s right brain involvement • Traumatisation involves the right hemisphere (feelings, memories, attachment). • Inevitability of re-enactment of abuse in therapy. • Importance of reparation during the therapeutic process: saying sorry! Dissociation and Reflective function • Use of video or tape-recording in severely dissociated patients. > The development of mentalisation or mindfulness. Therapist’s survival • Safety of therapeutic setting • Importance of peer or other supervision because of likely-hood of re-enactment. • Secondary traumatisation is inhererent to this type of work and needs to be addressed at all levels: self care, case load, support. Complex PTSD Programme 90 Days of structured work - 600 hours Three One Month Phases : • Interactive Psycho-Education & Adjustment of Medication. • Individual Disclosure of the Trauma • Cognitive Restructuring and Problem Solving CPTSD Programme content: • Multimodal Multidisciplinary Assessment Protocol • Group cohesion and boundary setting • Highly structured work schedule • Therapeutic Milieu • Psychoeducation – Trauma, Coping, Relationships • Medications • Disclosure on an individual basis • Cognitive restructuring / CBT • Behavioural Techniques • Discharge planning and Liaison Outcome Subject Data • • • • • • 34 (consecutive) patients entered programme Small groups 4 to 6 30 patients completed programme Mean age 26.2 years (r=17-45). 27 female; 3 male. 4 did not finish: 2 became too dangerous to self or staff. 2 were afraid to get better! Results: Open outcome data first 30 patients: Parametric and non-parametric statistics 90-Day Programme Outcome 60 50 40 CAPS- Intensity BDI GHQ 30 20 10 0 1 2 3 4 Results: Open outcome data first 30 patients: Parametric and non-parametric statistics 90-Day Programme Outcome Function 4 3.5 3 2.5 Social Function Occupational Function 2 1.5 1 0.5 0 1 2 3 4 Other findings Of first 25 patients: • 18 were transferred directly from inpatient wards where they had been treated cumulatively for 27 years (average 2 years 1 month) • At follow-up one patient was returned to hospital, the rest spent cumulatively 1 year 3 months in hospital • Self harm, eating disorders, OCD much improved. • Several got employment for first time in years or went to full or part-time education. Other findings Of first 25 patients: • 18 were transferred directly from inpatient wards where they had been treated cumulatively for 27 years (average 2 years 1 month) • Estimate have saved approx £1.2 million on admission times. • At follow-up one patient was returned to hospital, the rest spent cumulatively 1 year 3 months in hospital • Self harm reduced by 95%, eating disorders, OCD much improved. • Several got employment for first time in years or went to full or part-time education. The Dene: Forensic Service Medium Secure Hospital for Women Elizabeth Anderson Ward: Personality Disorder and Trauma Unit Strategy • Stabilization • Disclosure / Working through • Cognitive restructuring Rolling Programme • Assessment Protocol • Therapeutic Milieu / General Adult Ward • Dialectic Behaviour Therapy Skills groups and individual treatment • Open admission / rolling group programme • Trauma Psychoeducation Groups • Medications • Disclosure / Therapy on an individual basis • Cognitive restructuring • CBT, Behavioural, Body Therapy Groups • Rehabilitation / Discharge planning and Liaison DBT • Promotes team working in MDT • Promotes validates the patient • Promotes boundaried response in times of crisis eg DSH • Outcome studies: good results for borderline personality disorder • Limited outcome studies • Expensive to train Conclusions • CPTSD useful diagnostic frame work? • Interventions Evidence Base? Complex PTSD Disturbance on Three Dimensions • • Symptoms of : PTSD Somatic Affective Dissociation (reach psychotic intensity) Characterological Changes of: Control: Traumatic Bonding Lens of Fear Relationships: Lens of extremity-attachment versus withdrawal Identity Changes: Self structures Internalized images of stress Malignant sense of self Fragmentation of the self • Repetition of Harm To the self - faulty boundary setting By others - battery, abuse Of others - become abusers Deliberate self harm Conclusions: CPTSD – A useful diagnostic framework: • Very easy to mis-diagnose – few understand the concept of CPTSD. • Easy to label patient as Borderline PD and say they are untreatable • Easy to acknowledge co-morbid syndromes that are more conventional such as psychotic depression • Easy to diagnose schizophrenia / schizoaffective disorder. Post Script Special groups: • Veterans • Refugees Its not just about social support its about good enough attachments as well Why is Working With Veterans Complicated? Mental health problems can arise from a variety of causes in Veterans: • Pre service vulnerabilities – many join to escape a difficult life situation, poor education levels, IQ? • Military life itself – instutionalization, alcohol, family issues; bullying, non-operational occupational mental health injury; Operational service – traumatic exposure: single / multiple • Earlier onset of physical disorders related to military life – mainly orthopaedic including chronic pain / ENT problems; Physical disorders associated with mental health illness • Leaving the service and adjusting to civilian life – institutionalisation Loss of attachments • Help seeking Issues surrounding being macho, avoidance of seeking help, lack of understanding of and by civilians, shame, stigma, guilt, you were not there etc • Combination of the above The Needs of the Combat Stress Population: Clinical Audit Data All audits 2005-2009 N=608 % Significant Physical illness 71 Physical injury during military service 48 History of Psychiatric illness diagnosed prior to contact with Combat Stress as a measure of chronicity 80 Multiple exposure to military psychological trauma 92 Present and past history of alcohol and drug dependence and abuse 69 Significant attachment difficulties in childhood / adolescence incl CSA and other abuse 52 Commonest diagnosis PTSD 75 (N=508) Reading list • Briere & Scott (2006) Principles of Trauma Therapy. A guide to symptoms evaluation and treatment. Thousand Oaks, CA Sage. • johnbriere.com • Briere & Langtree (2008) Integrative treatment of complex trauma for adolescents (ITCT-A). Recommended reading • Busuttil, W. (2009) Complex PTSD: A useful diagnostic frame work? Psychiatry, 8:8, 310-314. • Effective treatments for PTSD. ISTSS Practice Guidelines (2009) eds Foa, E Keane & Friedman, M J. Guilford Press: New York. • Innovative Trends in Trauma Treatment Techniques. (2007) (eds M B Williams & J Garrick). Howarth Press: New York, USA. • M Nasser, K Baistow & Treasure J (2007)When the Body Speaks its Mind. The Interface between the Female Body and Mental Health. Routledge: London. • Luxenberg, T., Spinazolla, J., Hidalgo, J., Hunt, C. & Van der Kolk, B. (2001). Complex Trauma and Disorders of Extreme Stress (DESNOS) Part Two: Treatment. Directions in Psychiatry, 26, pp. 395-414. • Van der Kolk, B., Roth, S, Pelcovitz, D., Sunday S. & Spinazolla, J. (2005). Disorders of Extreme Stress: The Empirical Foundation of a Complex Adaptation to Trauma. Journal of Traumatic Stress, 18 (5), pp. 389-399. • References • Bloom, S. (1997) Creating Sanctuary. Toward The Evolution Of Sane Societies. London: Routledge, • Briere J & Scott C (2006) Principles of Trauma Therapy, A Guide to Symptoms, Evaluation and Treatment. Thousand Oaks, CA: Sage • Busuttil, W (2006) The development of a 90 day residential program for the treatment of Complex Post Traumatic Stress Disorder. Book Chapter (eds M B Williams & J Garrick ). In Innovative Trends in Trauma Treatment Techniques. Howarth Press: New York, USA. • Busuttil, W. (2007) Psychological trauma and Post Traumatic Stress Disorder. In: When the Body Speaks its Mind. The Interface between the Female Body and Mental Health. Pp 41-56, (eds M Nasser, K Baistow & J Treasure). Routledge: London. • Kinniburgh, K.L., Blaustein, M., Spinazzola, J et al (2005) Attachment, self regulation and competency. Psychiatric Annals 35, 424-430. • Sareen, J. Cox, BJ Goodwin, RD et al, (2005) Co-occurrence of Post Trauamtic Stress Disorder in a nationally representative sample. Journal of Traumatic Stress, 18, 313-322