Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
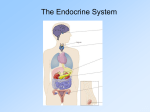
Role of endocrinic glands in regulation of body functions Pineal Gland produces Dimethyltryptamine Melatonin Function The pineal gland was originally believed to be a "vestigial remnant" of a larger organ (much as the appendix was thought to be a vestigial digestive organ). It was only after the 1960s that scientists discovered that the pineal gland is responsible for the production of melatonin, which is regulated in a circadian rhythm. Melatonin is a derivative of the amino acid tryptophan, which also has other functions in the Central Nervous System. The production of melatonin by the pineal gland is stimulated by darkness and inhibited by light. [7] The retina detects the light, and directly signals and entrains the suprachiasmatic nucleus (SCN). Fibers project from the SCN to the paraventricular nuclei (PVN), which relay the circadian signals to the spinal cord and out via the sympathetic system to superior cervical ganglia (SCG), and from there into the pineal gland. Thyroid gland produces Triiodothyronine (T3), the potent form of thyroid hormone Thyroxine (T4), a less active form of thyroid hormone Calcitonin Tetraiodothyronine (T4) or Thyroxine -Triiodothyronine (T3) a) helps regulate the metabolic rate of all cells and cell growth and tissue differentiation. Calcitonin a) influence the processing of calcium by bone cells by decreasing blood calcium levels and promoting conservation of hard bone matrix. Parathyroid gland produces Parathyroid hormone (PTH) Parathyroid Hormone (PTH) a) an antagonist to calcitonin and acts to maintain calcium homeostasis. b) acts on bone: causes more bone to be dissolved, yielding calcium and phosphate, which enters the bloodstream. c) acts on kidney: causes phosphate to be secreted by the kidney cells into the urine to be excreted. d) acts on intestinal cells: causes increased intestinal absorption of calcium by activating vitamin D. Thymus The thymus plays an important role in the development of the immune system, being the primary site of T cell maturation. The organ is most active between the late stages of gestation and early puberty, when most of the T cells an individual will carry for their lifetime are formed. With the onset of puberty the organ atrophies, gradually shrinking in size and function. The atrophy is due to the increased circulating level of sex hormones, and chemical or physical castration of an adult results in the thymus increasing in size and activity. In the two thymic lobes, lymphocyte precursors from the bone-marrow become thymocytes, and subsequently mature into T cells. Once mature, T cells emigrate from the thymus and constitute the peripheral T cell repertoire responsible for directing many facets of the adaptive immune system. Loss of the thymus at an early age through genetic mutation or surgical removal results in severe immunodeficiency and a high susceptibility to infection. The ability of T cells to recognize foreign antigens is mediated by the T cell receptor. The T cell receptor undergoes genetic rearrangement during thymocyte maturation, resulting in each T cell bearing a unique T cell receptor, specific to a limited set of peptide:MHC combinations. The random nature of the genetic rearrangement results in a requirement of central tolerance mechanisms to remove or inactive those T cells which bear a T cell receptor with the ability to recognise selfpeptides. Heart produces Atrial-natriuretic peptide (ANP) ANH’s primary effects is to oppose increases in blood volume or blood pressure; Also antagonist to ADH and aldosterone Stomach and intestines produce Cholecystokinin (CCK) Gastrin Neuropeptide Y (NPY) Secretin Somatostatin Liver produces Insulin-like growth factor (IGF) Angiotensinogen Thrombopoietin Islets of Langerhans in the pancreas produce Insulin Glucagon Somatostatin 1) Alpha cells secrete glucagons. 2) Beta cells secrete insulin and amylin 3) Delta cells secrete somatostatin. 4) F1 or PP1 cells secrete pancreatic polypeptides. Name of cells Product % of islet cells Function beta cells Insulin and Amylin 50-80% lower blood sugar 15-20% raise blood sugar alpha cells Glucagon delta cells Somatostatin 3-10% inhibit endocrine pancreas PP cells Pancreatic polypeptide 1% inhibit exocrine pancreas Insulin Action on carbohydrate metabolism: 1. Increase permeability of cell membrane to glucose. 2. Stimulate synthesis of glycogen. 3. Activate transformation of carbohydrates into fats 4. Decrease development of glucose from amino acids. Action on fat metabolism. 1. Decrease destruction of fat 2. Activates synthesis of fatty acids 3. Inhibit development of ketonic bodies. Action on protein metabolism. 1. Increase transmission of amino acids in cells. 2. Increase synthesis of proteins. 3. Decrease destruction of amino acids. The actions of insulin on the global human metabolism level include: Control of cellular intake of certain substances, most prominently glucose in muscle and adipose tissue (about ⅔ of body cells). Increase of DNA replication and protein synthesis via control of amino acid uptake. Modification of the activity of numerous enzymes (allosteric effect). Mechanism of glucose dependent insulin release -Glucagon 1. tends to increase blood glucose levels 2. stimulates gluconeogenesis in liver cells (transformation of fatty acids and amino acid into glucose). 3. increase glycogen conversion to glucose in liver cells. 4. stimulate lipolysis in liver. Increased secretion of glucagon is caused by: Decreased plasma glucose Increased catecholamines - norepinphrine and epinephrine Increased plasma amino acids (to protect from hypoglycemia if an all protein meal consumed) Sympathetic nervous system Acetylcholine Cholecystokinin Decreased secretion of glucagon (inhibition) is caused by: Somatostatin Insulin Function Glucagon helps maintain the level of glucose in the blood by binding to glucagon receptors on hepatocytes, causing the liver to release glucose stored in the form of glycogen - through a process known as glycogenolysis. As these stores become depleted, glucagon then encourages the liver to synthesize additional glucose by gluconeogenesis. This glucose is released into the bloodstream. Both of these mechanisms lead to glucose release by the liver, preventing the development of hypoglycemia. Increased free fatty acids and ketoacids into the blood Increased urea production -Somatostatin 1. Regulate the other endocrine cells of the pancreatic islets. Somatostatin is classified as an inhibitory hormone, whose main actions are to: Inhibit the release of growth hormone (GH) Inhibit the release of thyroid-stimulating hormone (TSH) Suppress the release of gastrointestinal hormones Lowers the rate of gastric emptying, and reduces smooth muscle contractions and blood flow within the intestine. Suppress the release of pancreatic hormones Gastrin Cholecystokinin (CCK) Secretin Motilin Vasoactive intestinal peptide (VIP) Gastric inhibitory polypeptide (GIP) Enteroglucagon (GIP) Inhibit the release of insulin Inhibit the release of glucagon Suppress the exocrine secretory action of pancreas. Somatostatin opposes the effects of Growth Hormone-Releasing Hormone (GHRH) Kidney produces Renin Erythropoietin (EPO) Calcitriol (the active form of vitamin D3) Skin produces Vitamin D3 (calciferol) Adipose tissue Leptin Estrogens (mainly estrone) Testes Androgens (chiefly testosterone) Testosterone Testosterone is a steroid hormone from the androgen group. Testosterone is primarily secreted in the testes of males and the ovaries of females although small amounts are secreted by the adrenal glands. It is the principal male sex hormone and an anabolic steroid. In both males and females, it plays key roles in health and well-being. Examples include enhanced libido, energy, immune function, and protection against osteoporosis. On average, the adult male body produces about twenty to thirty times the amount of testosterone that an adult female's body does. Effects In general, androgens promote protein synthesis and growth of those tissues with androgen receptors. Testosterone effects can be classified as virilizing and anabolic effects, although the distinction is somewhat artificial, as many of the effects can be considered both. Anabolic effects include growth of muscle mass and strength, increased bone density and strength, and stimulation of linear growth and bone maturation. Virilizing effects include maturation of the sex organs, particularly the penis and the formation of the scrotum in fetuses, and after birth (usually at puberty) a deepening of the voice, growth of the beard and axillary hair. Many of these fall into the category of male secondary sex characteristics. Testosterone effects can also be classified by the age of usual occurrence. For postnatal effects in both males and females, these are mostly dependent on the levels and duration of circulating free testosterone. Most of the prenatal androgen effects occur between 7 and 12 weeks of gestation. Genital virilization (midline fusion, phallic urethra, scrotal thinning and rugation, phallic enlargement) Development of prostate and seminal vesicles Early infancy androgen effects are the least understood. In the first weeks of life for male infants, testosterone levels rise. The levels remain in a pubertal range for a few months, but usually reach the barely detectable levels of childhood by 4-6 months of age. The function of this rise in humans is unknown. It has been speculated that "brain masculinization" is occurring since no significant changes have been identified in other parts of the body. Early postnatal effects are the first visible effects of rising androgen levels in childhood, and occur in both boys and girls in puberty. Adult-type body odour Increased oiliness of skin and hair, acne Pubarche (appearance of pubic hair) Axillary hair Growth spurt, accelerated bone maturation Fine upper lip and sideburn hair Advanced postnatal effects begin to occur when androgen has been higher than normal adult female levels for months or years. In males these are normal late pubertal effects, and only occur in women after prolonged periods of excessive levels of free testosterone in the blood. Phallic enlargement (including clitoromegaly) Increased libido and erection frequency Pubic hair extends to thighs and up toward umbilicus Facial hair (sideburns, beard, moustache) Chest hair, periareolar hair, perianal hair Subcutaneous fat in face decreases Increased muscle strength and mass Deepening of voice Growth of the adam's apple Growth of spermatogenic tissue in testes, male fertility Growth of jaw, brow, chin, nose, and remodeling of facial bone contours Shoulders widen and rib cage expands Completion of bone maturation and termination of growth. This occurs indirectly via estradiol metabolites and hence more gradually in men than women. Adult testosterone effects are more clearly demonstrable in males than in females, but are likely important to both sexes. Some of these effects may decline as testosterone levels decline in the later decades of adult life. Maintenance of muscle mass and strength Maintenance of bone density and strength Libido and erection frequency Mental and physical energy Ovarian follicle Estrogens (mainly estradiol) Corpus luteum Progesterone Estrogens (mainly estradiol) Placenta (when pregnant) Progesterone Estrogens (mainly estriol) Human chorionic gonadotropin (HCG) Human placental lactogen (HPL) Somatostatin is secreted not only by cells of the hypothalamus but also by delta cells of stomach, intestine, and pancreas. It binds to somatostatin receptors. Somatostatin Somatostatin is classified as an inhibitory hormone, whose main actions are to: Inhibit the release of growth hormone (GH) Inhibit the release of thyroid-stimulating hormone (TSH) Suppress the release of gastrointestinal hormones Gastrin Cholecystokinin (CCK) Secretin Motilin Vasoactive intestinal peptide (VIP) Gastric inhibitory polypeptide (GIP) Enteroglucagon (GIP) Lowers the rate of gastric emptying, and reduces smooth muscle contractions and blood flow within the intestine. Suppress the release of pancreatic hormones Inhibit the release of insulin Inhibit the release of glucagon Suppress the exocrine secretory action of pancreas. Somatostatin opposes the effects of Growth Hormone-Releasing Hormone (GHRH) Gonadal production of steroids. Only the ovaries have high concentrations of the enzymes (aromatase) required to produce the estrogens estrone and estradiol.