Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
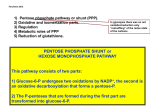
Good Afternoon! Screening Newborns too? Lorna Ramos-Abad,MD Dept. of Pediatrics UP College of Med-Phil Gen Hospital OBJECTIVES To increase awareness among practitioners about the availability of newborn screening in the Philippines To discuss briefly the conditions included in the newborn screening panel To highlight important provisions in the NBS act What is Newborn Screening? In most developed countries: – An integral part of routine newborn care As routine as Vitamin K injection or Cord Care In the Philippines: – It is now recognized as part of the standard newborn care Newborn Screening:Rationale early identification of congenital metabolic disorders that can lead to mental retardation or death if not treated involves collection of a few drops of blood by heel prick after the first 48 hours of life How is Newborn Screening Performed? Blood sample collection (>24 hours of life in term newborns) Analysis for the presence of the disorders screened (NIH laboratory) Positive Negative Confirmatory Test No further testing Positive Appropriate treatment and referrals Which disorders are screened? In the Philippines: Congenital Adrenal Hyperplasia (CAH) – 21 hydroxylase deficiency Congenital Hypothyroidism (CH) – Primary Congenital Hypothyroidism Glucose 6-Phosphate Dehydrogenase (G6PD) deficiency Galactosemia Phenylketonuria (PKU) MAGNITUDE OF THE PROBLEM Local prevalence of these disorders * Condition No. of Confirmed Cases Incidence rates Estimated no. of Babies Affected Annually (Assuming a cohort of 2.0M newborns) CH 130 1:3,065 594 CAH 68 1:5,860 337 GAL 4 1:99,618 22 PKU 4 1: 9,618 29 G6PD Deficiency 5,666 1:57 33,334 TOTAL 5,872 34,316 CLINICAL MANIFESTATIONS AT BIRTH DISORDER CAH APPEARANCE AT BIRTH Hyperpigmentation Ambiguous Genitalia in female infants CH Normal GAL Normal PKU Normal G6PD Deficiency Normal When do typical signs and symptoms appear? DISORDER CAH CH GOLDEN PERIOD 7-14 days 4 weeks Gal 2 weeks PKU 3 weeks G6PD deficiency On exposure to specific agents causing hemolysis What happens to unscreened and untreated babies? Disorder Screened CAH UNSCREENED, UNTREATED CH Severe Growth and Mental Retardation GAL Death or Cataracts PKU Severe Mental Retardation G6PD Deficiency Severe Anemia, Jaundice, Kernicterus Death What is CONGENITAL ADRENAL HYPERPLASIA? Steroidogenesis Cholesterol 17 OH Pregnenolone 3HSD Progesterone 17OHP 11 Deoxycortisol 11 hydroxylase Corticosterone P450c11AS ALDOSTERONE DHEAS Androstenedione 17 HSD P450c21 11 DOC P450c17 Pregnenolone P450c17 P450scc CORTISOL TESTOSTERONE CAH, Salt Losing Clinical Manifestations – Increased pigmentation – Ambiguous genitalia in female infants – Poor suck, weak cry – Vomiting, excessive urination, dehydration – Irritability and seizures – Failure to thrive – Hypotension, shock – Coma Congenital Adrenal Hyperplasia Late Manifestations – Precocious puberty – “Skin Puberty”: pubic hair growth, oily skin, “body odor" – Dark skin color – Short adult stature Congenital Hypothyroidism A deficiency in serum concentration of free thyroid hormone (fT4) Transient (10%) or permanent (90%) Forms: Primary (most common) or Secondary or Tertiary Congenital Hypothyroidism Clinical Manifestations – Prolonged jaundice – Inactive defecation – Umbilical Hernia – Hypotonia – Skin: rough and dry Pallor, coldness, hypothermia, edema – “Rough” facial features Edema, flat nasal bridge, enlarged tongue – Open fontanelles – Delayed overall development Congenital Hypothyroidism Late Manifestations – Mental retardation – Growth retardation – Delayed skeletal maturation – Delayed dental development and tooth eruption – Delayed puberty Galactosemia Galactose – Component of dietary sugars – Converted to GLUCOSE for energy storage (glycogen) and energy production Galactosemia results from a deficiency of Galactose-1phosphate uridyltransferase (GALT) – Enzyme responsible for converting galactose to glucose Galactosemia Clinical Manifestations develop a few days to two weeks AFTER INITIATION OF MILK FEEDINGS Poor suck Vomiting, occasionally diarrhea Jaundice Lethargy, weakness, coma Septicemia (E. coli) Later: excess galactose deposits in tissues Liver Hepatomegaly Edema Ascites Cirrhosis of the liver Lens Cataracts Brain Mental retardation Kidney Growth failure Galactosemia (Baby L) at 4 months at 1 year old Phenylketonuria Phenylalanine Essential amino acid found in most protein diets Tyrosine Produced from phenylalanine Component of substances that regulate body functions (hormones/ pigment) Inefficient production of tyrosine from phenylalanine Complete absence or profound deficiency of phenylalanine hydroxylase (PAH) enzyme activity Phenylketonuria Very high elevations of blood Phenylalanine – Excessive amounts of waste products of phenylalanine (phenylketones) in the urine Gives the urine a characteristic “mousy” odor Low serum levels of tyrosine – Disturbance in hormone and pigment production Phenylketonuria Clinical Manifestations – Vomiting – Hyperactivity – Seizures and hypertonia – Musty or mousy urine odor – Light hair and skin color – Seborrheic or eczematoid rash – Mental retardation Persistent Benign Hyperphenylalanemia (Baby MD) at 5 months at 1 year and 10 mos. G6PD Deficiency Function of G6PD – Certain food and drug have oxidant properties that causes cell damage Produce H2O2 and other reactive oxidizing products (OH+) – In the red blood cells (RBC), the only mechanism to neutralize oxidative substances is through the G6PD activity Without G6PD, RBC’s undergo HEMOLYSIS when exposed to oxidative stress! OXIDATIVE AGENTS LEADING TO HEMOLYSIS IN G6PD Deficiency Drugs Sulfonamides, quinolones, chloramphenicol, Vitamin K Chemicals Mothballs Food Fava beans Infection CLINICAL MANIFESTIONS OF G6PD Deficiency Acute Hemolytic crisis Anemia Decreased oxygen delivery Enlarged spleen Increased bilirubin Jaundice, tea colored urine Accumulation in tissues – Brain • Kernicterus – Gall bladder • Gallstones Screening and Confirmatory Tests DISORDER SCREENING TEST CONFIRMATORY TEST 17 OHP 17 OHP TSH ↓T4 ↑TSH Galactose ↓GALT activity Phenylketonuria (PKU) Phenylalanine ↓PAH activity Glucose 6-Phosphate Dehydrogenase (G6PD) Deficiency G6PD activity ↓G6PD activity Congenital Adrenal Hyperplasia (CAH) Congenital Hypothyroidism (CH) Galactosemia (GAL) Treatment Disorder CAH CH GAL PKU G6PD Deficiency Treatment Supplementation Glucocorticoid, mineralocorticoid, NaCl Supplementation Thyroid Hormone Avoidance Galactose, Lactose Avoidance Protein diet Avoidance Oxidative drugs, food and chemicals Enactment of the Newborn Screening Act of 2004 (April 6, 2004) Signing of the Implementing Rules and Regulation of RA 9288 (October 5, 2004) Highlights of RA 9288 Institutionalize the National Newborn Screening System – Section 2 Ensure that every baby born in the Philippines is offered the opportunity to undergo NBS Defining DOH as the lead agency for the implementation of NBS – Section 10 Creation of an Advisory Committee on NBS (ACNBS) – Section 11 DOH,DILG, NIH, NSRC, CWC, 3 reps (Pediatrics, Obstetrics, Midwife, Nurse, Family physician, Endocrinology) Highlights of RA 9288 Establishment and accreditation of the Newborn Screening Centers (NSC) – Section 12 Establishment of the Newborn Screening Reference Center (NSRC) – Section 13 Highlights of RA 9288 Obligation to inform – Section 5 Who will inform? – Any health practitioner who delivers, or assists in the delivery of a newborn What information? – Availability, nature and benefits of NBS Performance of Newborn Screening – Section 6 After 24 hours of life but not later than 3 days Sick neonates in ICU must be tested by the 7th day of life – Regardless of weight and age of gestation Highlights of RA 9288 Role of Health Institutions – Section 9 DOH and PHIC shall require health institutions to provide newborn screening services as a condition for licensure and accreditation • Hospitals, Health infirmaries, Health Centers, Lying-In centers or Puericulture centers with obstetrical and pediatric services – Section 14- A Serve as collecting health units for blood samples Establish a Newborn Screening Team • Information, education, communication, screening, recall and management of identified cases • Section 21-A All collecting health facilities throughout the country shall have NBS Specimen Collection Kits AT ALL TIMES!!! What is the cost of newborn screening? GIVING UP 1.5 sticks every day for 1 year Newborn Screening Fee P600 2 bottles every month for 9 months 1 bottle of coke every week for 1 year 2 cell cards in 9 months Missing 55 days of daily lotto bet Cost of Care : 1st year of life CONDITION IF SCREENED AND TREATED IF NOT SCREENED CH P10 a day (thyroid hormone) P 195 a day CAH P 1.34 –134 a day (steroids) P 1073 a day GAL P 35 (soy formula) P 410 a day PKU P 44 (low protein formula) P 6,492 a day None P 84 a day G6PD Deficiency *UP-PGH Service Ward 2002 SAVING 34,000 BABIES A YEAR FROM MENTAL RETARDATION AND DEATH!!! IS MORE THAN ENOUGH REASON TO SCREEN BABIES Thank you for listening!