Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
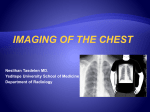
Pneumonia, Atelectasis & Effusions Normal Chest Good Inspiration Sharp Cardiac and Mediastinal Borders Sharp Costophrenic Angles Normal Pulmonary Vascularity Early CHF Cephalization of pulmonary vasculature Kerley lines Haziness of pulmonary vascular shadows Pleura effusions Severe CHF Diffuse Alveolar Edema Air Bronchograms Pleural Effusions Prominent Central Pulmonary Vasculature Lobar Pneumonia Most common gram positive pneumonia 90% community acquired Organism: strep pneumoniae Tends to affect elderly, immunocompromised, alcoholics, sickle cell patients Inflammatory edema in alveoli spread via pores of Kohn to more lateral alveoli Right Upper Lobe Consolidation Right upper lung zone density Air bronchograms No mediastinal shift or hemidiaphragm elevation Right Middle Lobe Consolidation Lingular Consolidation Hazy left lower lung zone opacity Loss of the left heart border Left hemidiaphragm still visible No evidence of volume loss Lingular Consolidation Triangular density projecting over the heart Small left pleural effusion Left Lower Lobe Consolidation Left lower lung zone opacity Loss of the left hemidiaphragm No significant volume loss or meniscus Left Lower Lobe Consolidation Left lower lobe opacity Major fissure not displaced Loss of left hemidiaphragm Atelectasis Evidence of volume loss Elevation of hemidiaphragm Displacement of fissures Crowding of ribs Compensatory emphysema Affected lung more opaque Crowding of bronchi Right Upper Lobe Atelectasis Elevation of the right hemidiaphragm Upward displacement of the minor fissure Increased triangular density abutting the right superior mediastinum Right Upper Lobe Atelectasis Common causes include Central obstructing mass Mucus plugging Right Middle Lobe Atelectasis Ill defined density abutting the right heart border Could be right middle lobe atelectasis or pneumonia Obtain lateral for confirmation Right Middle Lobe Atelectasis Triangular density projecting over the heart Downward displacement of the minor fissure Left Upper Lobe Atelectasis Increased veil like opacity within the left hemithorax Elevation of the left hemidiaphragm Left Upper Lobe Atelectasis Crescentic increased density abutting the anterior chest Anterior displacement of the major fissure Left Lower Lobe Atelectasis Triangular density behind the heart Loss of the medial hemidiaphragm Elevation of the left hemidiaphragm Left Lower Lobe Atelectasis Increased density over the lower thoracic spine Loss of the left hemidiaphragm Posterior and inferior displacement of the major fissure Pleural Effusions Blunting of the costophrenic angles Mediastinal shift if large enough Lateral decubitus film is very sensitive for detection of pleural effusion 10cc Pleural Effusions Obscuration of the hemidiaphragms 175cc can be hidden before being seen laterally Left pleural effusion can sometimes be estimated with help of gastric bubble Pleural Effusions Blunting of the posterior costophrenic angle Subpulmonic Effusion Lateralization of the diaphragm apex Elevation of the hemidiaphragm Loculated Effusions Increased opacity over the right hemithorax No blunting of the costophrenic angle Density does not correspond to lobar anatomy Diaphragm and heart still visible Loculated Effusion Homogeneous density abutting the posterior chest wall with obtuse margins Sharp margin anteriorly Suspicious for empyema Loculated Effusion Homogeneous density abutting the right lateral chest wall Has a sharp medial margin Does not have a meniscus Self Test Subpulmonic Effusion Right Middle Lobe Atelectasis Normal Chest Large Right Pleural Effusion Left Upper Lobe Atelectasis Early CHF Right Upper Lobe Atelectasis Left Lower Lobe Pneumonia Loculated Effusion Right Upper Lobe Pneumonia