Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
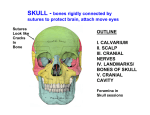
Cranium RTEC 233 Fall 2008 Week 1 & 2 Cranial Anatomy Calvaria Floor Frontal Ethmoid Occipital Sphenoid Left Parietal Left Temporal Right Parietal Right Temporal The regions of the Cranial Floor Anterior: extends form anterior frontal bone to the lesser wings of the sphenoid Middle: Extends from lesser wings to the apices of petrous ridges of temporal bone It is associated with frontal lobes of cerebellum Accommodates temporal lobes and associated neurovascular structures Posterior: deep depression posterior to petrous ridge which protects cerebellum, pons and medulla oblongata Frontal Bone Has a vertical and horizontal portion Vertical portion- forms the forehead and anterior part of the vault Horizontal portionforms roof of orbits, part of the roof of nasal cavity, and greater part of anterior cranial fossa. Parietal Bone Forms large part of sides of the cranium Forms posterior portion of the cranial floor Parietal eminence is used to measure width of head Occipital Bone Inferosuperior portion of calvaria Squamous portion is superior to inion Ext. occipital protuberance – prominent bulge Contains foramen magnum and articulates with atlas (C1) Ethmoid Bone Horizontal portion is called cribiform plate Vertical portion is called perpendicular plate 2 light spongy labyrinths Sphenoid Bone Resembles shape of a bat Consists of a body, 2 lesser wings, 2 greater wings, 2 pterygoid processes Contains Sella turcicaimportant for positioning errors Sella Turcica Lies in the MSP ¾” anterior & superior to EAM Deformity of the sella is often the only clue that a lesion exists intracranially Temporal Bone Divided in 3 parts Squamous: upper portion forming part of the wall of skull Mastoid: Posterior to EAM contains mastoid tip (process) Petrous: dense & houses organs of hearing and balance Thickest most dense bone in cranium Level of TEA Superior Cranium Visualized more clearly: Sphenoid Temporals Occipital Frontal Not well visualized: Ethmoid Parietals Copyright © 2003, Mosby, Inc . Lateral Cranium From this view you can visualize all the cranial bones Copyright © 2003, Mosby, Inc. Infant Sutures & Fontanels Anterior 2 Mastoids Close approx 2 years 2 Sphenoidal Close approx 2 years 1-3 months old Posterior 1-3 months Copyright © 2003, Mosby, Inc. Adult Sutures and Junctions Sutures: Coronal Sagittal Squamosal Lamboidal Junctions Bregma Lambda Pterion Asterion Copyright © 2003, Mosby, Inc. Lets compare Infant Adult Anterior fontanel Bregma Posterior fontanel Lambda Sphenoidal fontanels Pterions Mastoidal fontanels Asterions Anterior Cranium Not able to visualize: Occipital Ethmoid Able to visualize: Parietals Frontal Sphenoid Temporals . Copyright © 2003, Mosby, Inc Cranial Topography Surface Landmarks Mesocephalic: average Brachycephalic: Short and broad 47 degrees Width 80% or greater than length 54 degrees Dolichocephalic: long and narrow Width is less than 75% than the length 40 degrees Skull morphology Skull Positioning Lines Skull Topography Be able to locate the following landmarks: Glabella Inner canthus Outer canthus Nasion Infraorbital margin Acanthion Gonion Mental point External auditory meatus (EAM) Auricular point Top of ear attachment (TEA) Radiographic Landmarks Interpupillary line (IPL) Acanthiomeatal line (AML) Perpendicular line between pupils of eyes From acanthion to EAM Mentomeatal line (MML) From mental point (center of chin) to EAM Radiographic Landmarks Orbitomeatal line (OML) Infraorbitomeatal line (IOML) From outer canthus to EAM From infraorbital margin to EAM Glabellomeatal line (GML) From glabella to EAM Positioning Aids Use any straightedge: •Straw •Pen/pencil Most Common Positioning Errors Rotation Tilt Excessive Flexion Excessive Extension Incorrect CR angle Rotation Tilt Copyright © 2005, Mosby, Inc. Indications for Cranial Radiography Skull fractures Neoplasms Linear Depressed Basal skull Metastases Osteolytic Osteoblastic Combo of both Gunshot wounds Multiple myeloma Pituitary Adenomas Paget’s Disease Subdural hematoma Acoustic neuroma http://www.skullbaseinstitute.com/video_ pituitary_tumor.htm http://www.skullbaseinstitute.com/video_a coustic_neuroma.htm Disinfect the Table or Bucky!! Cleanliness Hair and skin of face are naturally oily; illness often increases oiliness Cranial procedures require direct contact of patient’s face with VBS Clean device after each patient Wash your hands!!! Radiation Protection Collimate to anatomy of interest Shield gonads/abdomen of pediatric patients and those of reproductive age Shield thyroid and thymus of pediatric patient when doing so will not interfere with demonstration of anatomy of interest Good communication and positioning skills reduce chance of need for repeat radiographs General Body Position Hyposthenic/asthenic patients usually need support at chest to elevate C-spine Helps prevent downward tilt of MSP Hypersthenic patients require radiolucent support at head Helps prevent upward tilt of MSP Hyposthenic/Asthenic Patients Hypersthenic Patients