Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
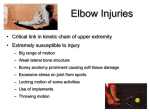
Chapter 15 The Elbow Complex Overview The elbow complex is an inherently strong and stable compound joint, which is enclosed within the capsule of the cubital articulation. The stability of the elbow complex, gives it very little in the way of compensatory adjustments, making it prone to overuse injuries The primary function of the elbow complex is to work together with the shoulder to position the hand for functional activities Anatomy The elbow complex is comprised of three distinct articulations: – The humeroulnar joint – The humeroradial joint – The proximal radioulnar joint Humeroulnar Joint A uniaxial hinge joint formed between the trochlear notch of the proximal ulna and the spool-shaped trochlea of the humerus The angulation of this joint forms the “carrying angle” The carrying angle is approximately 11-14° in males and 13-16° in females Humeroradial Joint A uniaxial hinge joint formed between the spherical capitellum of the humerus, and the concave head of the radius The design of this joint allows the elbow to flex and extend, and for the radius to rotate Proximal Radioulnar Joint The proximal (superior) radioulnar joint is a uniaxial pivot joint formed between the periphery of the convex radial head, and the fibrous osseous ring formed by the concave radial notch of the ulna The annular ligament forms 80% of the articular surface of the proximal radioulnar joint Joint Capsule The joint capsule of the elbow complex is thin but strong The capsule of the joint does not respond well to injury or prolonged immobilization, and often forms thick scar tissue, which may result in flexion contractures of the elbow Medial (Ulnar) Collateral Ligament The fan-shaped MCL is functionally the most important ligament in the elbow for providing stability against valgus stress, particularly in the range of 20-130° of flexion and extension There are three distinct components of the MCL: – Anterior bundle – Transverse bundle – Posterior bundle Medial (Ulnar) Collateral Ligament Anterior bundle – Anterior band The strongest and stiffest of the elbow collateral ligaments Primarily stabilizes the elbow against valgus stress in the ranges of 20-120° of flexion, and becomes a secondary restraint with further flexion Medial (Ulnar) Collateral Ligament Anterior bundle – The posterior band Taut beyond 55° of elbow flexion A secondary restraint to valgus stress at lesser degrees of flexion An equal co-restraint with the anterior band at terminal elbow flexion A primary restraint to passive elbow extension Medial (Ulnar) Collateral Ligament The transverse bundle – Also known as Cooper’s ligament – Fibers both originate and insert on the ulna and therefore have little role in elbow stability Medial (Ulnar) Collateral Ligament Posterior bundle – Appears to be a thickening of the posterior elbow capsule – Provides only secondary restraint to valgus stress at flexion beyond 90°. Lateral (Radial) Collateral Ligament Consists of: – – – – The The The The annular ligament fan-like radial collateral ligament accessory collateral ligament lateral ulnar collateral ligament The LCL functions to maintain the ulnohumeral and radiohumeral joints in a reduced position when the elbow is loaded in supination Annular Ligament The annular ligament functions to maintain the relationship between the head of the radius and the humerus and ulna Bursae The olecranon bursa is the main bursa of the elbow complex and lies posteriorly between the skin and the olecranon process Under normal conditions the bursa does not communicate with the elbow joint, although its superficial location puts it at high risk for injury from direct trauma to the elbow Elbow Flexors The prime movers of elbow flexion are the biceps, brachialis, and brachioradialis The pronator teres, flexor carpi radialis (FCR), and flexor carpi ulnaris (FCU), and the extensor carpi radialis longus (ECRL) muscles are considered as weak flexors of the elbow Elbow Extensors There are two muscles that extend the elbow: the triceps and the anconeus Forearm Pronators Pronator teres Pronator quadratus Flexor carpi radialis Forearm Supinators Biceps Supinator Cubital tunnel A fibro-osseous canal that contains the ulnar nerve – The floor of the tunnel is formed by the MCL – The roof is formed by an aponeurosis, the arcuate ligament – The medial head of the triceps constitutes the posterior border of the tunnel – The anterior and lateral borders are formed by the medial epicondyle and olecranon, respectively The volume of the cubital tunnel is greatest with the elbow held in extension Cubital Fossa The cubital fossa represents the triangular space, or depression, which is located over the anterior surface of the elbow joint, and which serves as an ‘entrance’ to the forearm, or antebrachium Cubital Fossa The contents of the fossa include: – The tendon of the biceps brachii lies as the central structure in the fossa – The median nerve – The brachial artery – The radial nerve – The median cubital or intermediate cubital cutaneous vein Nerves Ulnar Radial Median The Arcade of Fröhse The arcade of Fröhse is an inverted arched structure that lies within 1 cm distal of the fibrous edge of the ECRB and approximately 2 to 4 cm distal to the radiohumeral joint It represents the proximal border of the superficial head of the supinator, through which the radial nerve passes The Radial Tunnel/Supinator Canal The radial tunnel lies on the anterior aspect of the radius, and is approximately three to four finger breadths long, beginning just proximal to the radiohumeral joint, and ending at the site where the nerve passes deep to the superficial part of the supinator muscle Biomechanics Biomechanically, the elbow predominantly functions as an important link in the upper extremity kinetic chain, allowing the generation and transfer of forces which occur in the upper extremity. Humeroulnar Joint The resting, or open pack, position for the humeroulnar joint is 70° of flexion with 10° of forearm supination The closed pack position is full extension and maximum forearm supination The capsular pattern is much more limitation in flexion than extension Humeroradial Joint The resting, or open pack, position of the humeroradial joint is extension and forearm supination The closed pack position is approximately 90° of elbow flexion and 5° of supination There is no true capsular pattern at this joint, although clinically an equal limitation of pronation and supination is observed Proximal Radioulnar Joint The resting, or open pack, position for the proximal radioulnar joint is 70° flexion and 35° of forearm supination The closed pack position is 5° of forearm supination The capsular pattern is minimal to loss of motion, with pain at the end ranges of pronation and supination Force Couples of the Elbow The triceps/biceps during arm extension and flexion Flexor carpi radialis (FCR), flexor carpi ulnaris (FCU), flexor digitorum communis (FDC)/Extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), extensor communis (EC) during wrist flexion and extension Force Couples of the Elbow Pronator teres, pronator quadratus/supinator during forearm pronation and supination Triceps/biceps, brachioradialis; pronator teres/supinator; FCR, FCU/ECRB, ECRL during activities requiring elbow stabilization Examination History – During the history, the clinician must determine the chief complaint and whether there is a specific mechanism of injury Where is the pain? Was there any antecedent trauma or overuse? Is there any paresthesia? What makes the symptoms better/worse Examination Systems Review – The clinician should be able to determine the suitability of the patient for physical therapy – If the clinician is concerned with any signs or symptoms of a visceral, vascular, neurogenic, psychogenic, spondylogenic or systemic disorder that is out of the scope of physical therapy, the patient should be referred to an appropriate healthcare provider Examination Observation – The affected elbow should be inspected for scars, deformities, and swelling – The clinician should observe the ‘carrying angle’ of the elbow and compare it to the other side Examination Palpation – Because they are superficial, most of the elbow structures are easily palpable, making it easier for the clinician to pinpoint the specific area of pain Examination Active range of motion with passive overpressure – It is important to determine how much range of motion (ROM) is necessary for the patient to perform his or her job and recreational activities – The patient is asked to perform active flexion, extension of the elbow, pronation and supination of the forearm, and wrist flexion and extension. The ranges are recorded Examination Resistive testing – In addition to all of the shoulder muscles that insert at or near the elbow (biceps, brachialis, triceps), the clinician must also test the muscles responsible for elbow flexion, and extension, forearm supination, pronation, and wrist flexion and extension Examination Functional assessment – A number of tests have been designed to assess elbow function Examination Passive articular motion testing – The – The – The – The ulnohumeral joint radiohumeral joint proximal radioulnar joint distal radioulnar joint Examination Stress tests – Medial (ulnar) collateral ligament (valgus test) – Lateral (radial) collateral ligament (varus test) Examination Special tests – Tennis elbow tests Cozen’s test Mill’s test – Golfer’s Elbow test – Cubital tunnel syndrome tests Elbow flexion Pressure provocative test – Tinel’s Sign (at the elbow) Intervention Strategies Acute Phase – Protection of the injury site – Restoration of pain-free range of motion in the entire kinetic chain – Improve patient comfort by decreasing pain and inflammation – Retard muscle atrophy – Minimize detrimental effects of immobilization and activity restriction – Maintain general fitness – Patient to be independent with home exercise program Intervention Strategies Functional Phase – Attain full range of pain free motion – Restore normal joint kinematics – Improve muscle strength to within normal limits – Improve neuromuscular control – Restore normal muscle force couples