Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
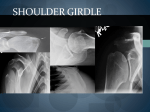
SHOULDER GIRDLE Standard Shoulder Views: *a. AP Internal Rotation *b. Grashey (oblique) *c. Scapular Y-view (oblique) *d. Axillary Lateral or Transthoracic Lateral/ Lawrence method (when pts. can’t lift arm) e. AP External Rotation or Neutral Rotation AP Rt Shoulder Internal Rotation * This image is clipping the end of the clavicle and scapula Structures shown: AP Shoulder * The entire scapula, clavicle and the proximal humerus Internal rotation shows lesser tubercle in profile * this is different then Merrill’s External vs. Internal Rotation Greater Tubercle External See arrow for greater tubercle Internal See arrow for lesser tubercle AP Internal Rotation: This view is taken with the arm internally rotated. The humeral head is rotated so that structures not seen in the external rotation view may now be seen. Note the following differences in the views: The greater tubercle is anterior on the humeral head and cannot be clearly seen (it is in the most lateral portion of the humeral head on the external rotation view). ****The lesser tubercle is seen medially (it is not seen on the external rotation view). The glenohumeral joint is still partially obscured by the humeral head. The entire clavicle and scapula should be on the film You should be able to identify the AC joint, coracoid process, acromion, clavicle, the scapula and glenohumeral joint. AP RT Shoulder Internal Rotation Bursitis AP Rt Shoulder Neutral Rotation What is wrong with this shoulder? AP Lt Shoulder ? Internal or external rotation Grashey Rt Shoulder Structures shown: Humeral head, open glenoid cavity and the neck of the scapula Grashey: Start with patient AP (standing is easier on the pt.) and roll onto affected shoulder about 45 degrees.* With arm internally rotated (some site use and external rotation) You want to get the glenoid cavity in profile You can cone in on this one! Structures shown : Joint space open between the humeral head and glenoid cavity (scapulohumeral joint) Is it open? Grashey Rt Shoulder No: roll patient up onto shoulder more Scapular Y Right Shoulder **Preferred R PA AP Trauma pt Y-view : PA oblique projection When the shoulder is being imaged to rule out dislocation or proximal humeral fracture, the patient’s humerus should not be moved. The PA method is the preferred method(less magnification) but when doing a trauma patient you should not stand them up or roll them PA so do them AP. The Y-view is taken by aligning the plane of the scapula parallel with the x-ray beams so that it can be seen "floating" over the thoracic rib cage. In a healthy patient, have their arm hanging down to their side, the humeral head should be in alignment with the glenoid fossa of the scapula. However, following a traumatic dislocation, leave the arm in the position it is in! The humeral head will not be resting in the glenoid fossa when dislocated Structures shown: the scapula ,coracoid, acromion and the humeral head You should be able to identify the scapula in profile, coracoid, acromion, humeral head as it overlies the glenoid fossa, the humeral shaft and the clavicle. Can you see the “Y”? What side of the scapula is the humeral head on? Posterior Coracoid Acromion Posterior Anterior Anterior Normal Anterior dislocation Posterior dislocation Did you know? Posterior shoulder dislocations, places the humeral head posterior, and beneath the acromion process Anterior shoulder dislocations, places the humeral head anterior, and beneath the coracoid Axillary Lateral Rt Shoulder inferior to superior superior to inferior Axillary Lateral View: The x-ray beam is directed either up into the axilla (inferior to superior), or from the superior aspect of the shoulder down through the axilla (superior to inferior). The axillary shows whether the humeral head is within, the glenoid fossa. Structures shown : Proximal humerus, Scapulohumeral joint, coracoid process, and the AC articulation. Do you have: Open scapulohumeral joint Coracoid process projected above the clavicle Lesser tubercle in profile and directed anteriorly AC joint projected through the humeral head **Is there extra soft tissue in the axilla (Breast tissue) Transthoracic Lt Shoulder pacemaker Fractured Anatomic Neck Transthoracic Lateral (Lawrence Method) Usually done on trauma patients Done in place of the axillary view Usually done as is. If patient is supine do supine, if patient is sitting up do sitting up. You need to raise the uninjured arm above the head. Need to get the unaffected shoulder up and out of the way. Ask patient if they can move the other arm first. Structures shown: Lateral projection of the shoulder and head of the humerus through the thorax. Fractured Head of Humerus Transthoracic Rt Shoulder Do you have: The proximal humerus on the image Can you see scapula, clavicle and humerus through the lung field Scapula superimposed over the thoracic spine Unaffected clavicle and humerus projected above the shoulder closest to the IR AP Rt Shoulder External Rotation AP External Rotation: ***not a protocol film This view is taken with the patient in the AP position either standing, sitting or laying down depending on the patient. The arm is externally rotated so that the thumbs points laterally. Structures shown: Entire clavicle ,scapula and proximal humerus ****The greater tubercle in the lateral aspect of the humeral head. Superior part of the humeral head obscures the glenoid fossa. Entire Scapula (the spine, borders and tip), and AC joint. The view of the coracoid process is head-on. Structures that you should be able to identify include the AC joint, coracoid process, acromion, glenohumeral joint, greater tubercle of the humerus and surgical neck of humerus. DID YOU KNOW? AP shoulder films are taken in internal and external rotation to improve visibility of components of the head of the humerus (the greater and lesser tubercles), the clavicle and scapula. This is a good overview of the shoulder. But: The Y-view and transthoracic view are used to evaluate for dislocations, where is the head of the humerus sitting compared to the joint space? AC joints Standard views: AP Bilateral AC Joints with out weights AP Bilateral AC Joints with weights AP Rt AC joint with out weights AP Lt Ac joint with out weighs AP Bilateral AC Joints With Out Weights with out wts The patient stands in the anatomical position and an AP film is taken that includes both AC joints (right and left) at the same time (2;8x10’s ,7x17, or 14x17 ). This allows comparison of the two joints. A second film is taken with the patient in the same position, but while holding weights in both arms(give the patient the weight very carefully). This is the "stress view", and helps in diagnosing AC joint separation by increasing the load that the joint has to bear. If there is ligamentous injury, the joint space will widen. The two spaces requiring careful evaluation are the (1)acromioclavicular joint space and the (2)coracoclavicular space. Both should be symmetric on right and left and should not be abnormally widened. Increased distances across the spaces indicate a degree of joint separation or sprain. The film from the previous slide was taken of a college football player who suffered an AC separation on the right. Note the widening compared to the left side. You should be able to see the following anatomical structures: bilateral: clavicles (distal ends if two films are taken), acromion, coracoid process, and humeral heads. One 14x17 cut in half AP Bilateral AC Joints With Out Weights 1 2 AP Bilateral AC Joints with weights Scapula Standard views: AP/Lateral AP Rt Scapula Lateral Rt Scapula Scapula AP: **Abducted arm (per patient’s condition) Structures shown: A true AP projection of the scapula shows the lateral portion of the scapula free of superimposition from the ribs and the rest of the scapula seen thru the ribs. AP RT Scapula RT * PA patient preferred Lateral Lateral Rt Scapula AP patient position RAO LPO Shows Rt Scapula Shows Rt scapula • Lateral:** (PA patient)RAO/LAO preferred (usually done upright) roll patient 45 to 60 degree toward affected side or (AP patient) RPO/LPO (usually done supine) roll pt. 15-25 degrees away from affected side • Structures shown: A lateral projection of the entire scapula. Scapular lateral border should not be superimposed on the ribs. ***Humerus should not superimposed the area of interest. Acromion process should be on film. OUCH! Scap “y”, Outlet and Lateral Scapula how do you tell them a part? Central ray: is it angled? 10-15 caudal for a outlet view. Where is it centered? The scapulohumeral joint or mid scapula What do they show? The whole scapula, the head of the humerus vs the joint or acromion and AC joint area What position is the arm in? Is it neutral for dislocation or is it moved to see the scapula? * I will not test you on the outlet view! Lateral scapula Arm out of the way Scap Y Arm relax Outlet Tube angle Clavicle Standard views: AP and AP axial Structures shown: Entire clavicle on one film. Even density from tip to middle to end. AP axial shows the same structures but most of the clavicle should be above the ribs and scapula. Clavicle should look more horizontal. AP Rt Clavicle AP Axial Rt Clavicle RT L AP Axial Lt clavicle AP Lt clavicle AP axial Why do we angle? AP Lt clavicle AP Axial Lt clavicle