Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
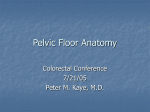
Female Pelvic Anatomy • The hip bone is originally made up of three bones that have fused: 1)ilium, 2)ischium and 3)pubis. These come together at the acetabulum. • The pelvic brim extends from promontory of the sacrum, arcuate line of the ilium, pectineal line and pubic crest. Some people divide the pelvis into a greater (or false) pelvis and lesser (or true) pelvis. • No muscle crosses the pelvic brim. If they did, they would be in the way during childbirth. Ligaments of the Pelvis The sacrotuberous and sacrospinous ligaments complete the greater and lesser sciatic foraminae The inlet to this canal is at the level of the sacral promontory and superior aspect of the pubic bones. The outlet is formed by the pubic arch, ischial spines, sacrotuberous ligaments and the coccyx. The ideal or gynaecoid pelvis is recognised by its well-rounded oval inlet and similarly uncluttered outlet The inlet has its longest dimension from side to side, whereas at the outlet the longest dimension is anteroposteriorly The upper sacrum is stabilised by the illiolumbar ligaments via its attachment to the fourth and fifth lumbar vertebra and the lower sacrum by the sacrospinous and sacrotuberous ligaments attachments to the posterior iliac spines and ischial tuberosities. During pregnancy, the elevated levels of oestrogen, progesterone and relaxin play a major role in increasing the laxity of the pelvic girdle joints. The hormonal levels do return to normal in the weeks following childbirth, but the time taken will also be affected by breastfeeding. By 3 to 6 months postnatal, the pelvic girdle should return to its prepregnant state; it may need external stabilisation during this period. An increase has been found in the width of the symphysis pubis from 4 mm to 9 mm in asymptomatic women on X-ray . The separation of less than 1cm should be considered normal, a greater separation being considered a partial or complete rupture; this may be up to 12 cm. resulting in tension and pain at the sacroiliac joints or symphysis pubis, or both. in the full squatting position; it has been estimated that the area of the outlet can be increased by as much as 28% in this way . In squatting, the femora apply pressure to the ischial and pubic rami, thus producing separation outward at the symphysis pubis and an upward and backward rotation of the sacrum. THE PELVIC FLOOR AND MUSCLES OF THE PELVIS The puborectalis is actually a part of the pubococcygeus muscle that wraps around the posterior aspect of the rectum forming a sling that holds the rectum forward in the pelvis. The pubococcygeus and iliococcygeus muscles make up the levator ani. The muscles of the levator ani are important supportive muscles for the midline organs of the pelvis. Any weakness in these muscles can cause clinical problems of urinary or fecal incontinence. The levator ani muscles otherwise known as the pelvic diaphragm or pubovisceralis (pubococcygeus) and iliococcygeus, are composed of striated muscle fibre. They are covered by fascia on their superior and inferior aspects. The anterior midline cleft in the muscles is known as the urogenital hiatus, through which the urethra, vagina and anorectum pass. The perineal membrane is sometimes called the urogenital diaphragm, or the triangular ligament. It lies inferior to the levator ani and attaches the edges of the vagina to the ischiopubic ramus, provides lateral attachments for the perineal body and assists in the support of the urethra. It is suggested that it has a greater supportive function when the levator ani muscles are relaxed. levator ani is considered as several separate muscle parts: •pubovaginalis •coccygeus •iliococcygeus •pubococcygeus •Puborectalis origin: from a tendinous arch between the pubis and ischial spine on the internal surface of the pelvis insertion: perineal body external wall of anal canal anococcygeal ligament coccyx Pubovaginalis originate from the posterior pelvic surface of the body of the pubis bone. Fibres pass inferiorly, medially and posteriorly. inserts into the central perineal tendon posterior to the vagina. The levator ani muscle seen from above looking over the sacral promontory (SAC) showing the pubovaginal muscle (PVM). The urethra, vagina, and rectum have been transected just above the pelvic floor. PAM = puboanal muscle; ATLA = arcus tendineus levator ani; and ICM = iliococcygeal muscle The arcus tendineus levator ani (ATLA); external anal sphincter (EAS); puboanal muscle (PAM); perineal body (PB) uniting the 2 ends of the puboperineal muscle (PPM); iliococcygeal muscle (ICM); puborectal muscle (PRM). The arcus tendineus fascia of the pelvis (ATFP) is a linear fascial thickening of the obturator fascia attached anteriorly to the pubic bone and posteriorly to the ischial spine and is believed to be of great importance in the continence mechanism levator ani Muscle showed that it was made up of large diameter type I (slow twitch) and type II (fast twitch) striated muscle fibres, with muscle spindles observed. Muscle activity may be recorded by electromyograph (EMG) from the levator ani muscle ‘at rest’ and even in sleep; presumably the type I fibres are responsible for this. By contrast, type II fibres are highly fatiguable but produce a high order of power on contraction. All these facts support the contention that the levator ani muscle is a skeletal muscle adapted to maintain tone over prolonged periods and equipped to resist sudden rises in intra-abdominal pressure, as for example on coughing, sneezing, lifting or running. It has been shown that there is reflex activity such that a fast-acting contraction occurs in the distal third of the urethra, which contributes to the compressive forces of the proximal urethra during raised intra-abdominal pressure The perineal body is a central cone-shaped fibromuscular structure which lies just in front of the anus. The cone is about 4.5 cm high and its base, which forms part of the perineum, is approximately 4 cm in diameter. Anteriorally it fuses with the vaginal wall, the superficial transverse perineal muscles, the perineal membrane and the levator ani muscles insert into it. The perineal body also affords support to the posterior wall of the vagina. The integrity of the perineal body and its connections have been thought to be of considerable importance in the supportive role of the pelvic floor. This explains the concern that obstetricians have had for the welfare of the perineal body in labour, particularly in the second stage when, toward delivery, the pelvic floor stretches considerably and provides a gutter to guide the foetal head towards and down the birth canal.