Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
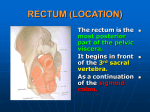
Pelvic Anatomy District I ACOG Medical Student Education Module 2011 Gynecologic Viscera Uterus: thick, muscular organ Derived from the fusion of the paramesonephric (mullerian) ducts. These ducts also form the upper 2/3 of the vagina and the fallopian tubes. Divided into 3 segments: fundus, lower segment and cervix. 3 layers: serosa, myometrium (smooth muscle), and endometrium. Gynecologic Viscera Fallopian tubes: 10-14 cm in length, <1 cm in diameter. Isthmus - 1 mm in diameter - perfect spot for tubal ligation. Ampulla - 6mm in diameter fertilization occurs here as well as most ectopics. Ligamentous Support Round Ligament: Fibrous and muscle tissue Anterior to the fallopian tubes Correlate with the male gubernaculums They extend laterally, cross the external iliac vessels, and enter the internal inguinal ring, and insert in the labia majora. Sampson’s artery, a branch of the uterine artery, runs along the length of the round ligament. Ligamentous Support Broad Ligament: Double reflection of the peritoneum, draped over the round ligaments. Cardinal Ligament: Found at the base of the broad ligament. Provides the main support for the uterus and cervix. It attaches to the cervix and extends laterally, connecting to the endopelvic fascia. Ligamentous Support Uterosacral Ligaments: Provide minor cervical support. Originate from the upper posterior cervix, travel around the rectum bilaterally, and fan out to attach to the 1st - 5th sacral vertebrae. Gynecologic Viscera Ovaries: Supported along the lateral pelvic sidewalls by the ovarian ligaments (attaching to the posteriolateral aspect of the uterus), the mesovarium (anastomotic region of the uterine and ovarian vessels), and the infundibulopelvic ligament (“The IP”), which are reflections of the broad ligament attaching the ovaries to the lateral pelvis. Ovaries They rest in the ovarian fossa, immediately adjacent to the iliac vessles and the ureters. They contain 3 distinct cell populations: Germ cells Stromal cells - tightly packed around developing follicles and secrete hormones. Epithelium Bladder and Rectum Don’t forget they are close by… Bladder is anterior to the uterus. Ureters originate in the renal calyces and insert in to the inferior bladder at the trigone. Careful attention to the ureters path in the pelvis is essential for dissection in gynecologic surgery. Key Points of the Ureter In the pelvis the ureter runs medial to and parallel with the internal iliac artery. Uterine artery crosses over the ureter (water under the bridge). The remaining 2-3cm of the ureter passes through the cardinal ligament into the bladder. Rectum Lies posterior to the uterus following the curvature of the sacrum. Blood Supply Majority originates from the internal iliac artery (aka: hypogastric artery). Additional supply comes from the ovarian arteries, the inferior mesenteric artery, and the external iliac artery. Common iliac --> external and internal iliac External becomes the femoral artery Internal iliac --> anterior and posterior divisions Posterior division - rarely seen in pelvic surgery, has three branches that supply the gluteal region: – Superior gluteal – Iliolumbar – Lateral sacral arteries Anterior division: Uterine Vaginal Superior, Middle, and Inferior Vesicals Middle and Inferior Rectal Obturator Inferior gluteal Internal Pudendal Obliterated umbilical arteries During retroperitoneal surgery the primary branches identified are the: Superior vesical artery Uterine artery Obturator artery Ovarian arteries Originate directly from the aorta, inferior to the renal arteries. Most frequently identified at the IP ligament. Ovarian veins: Left ovarian vein drains into the left renal vein Right ovarian vein drains directly into the inferior vena cava. Lymph Drainage Cervical Cancer: Drains 1st to the parametrial nodes --> obturator nodes --> pelvic nodes --> para-aortic Uterine Cancer: Drains 1st to the pelvic nodes or para-aortic. Ovarian Cancer: Can metastasize to either the pelvic or paraaortic nodes. Pelvic Support Pelvic diaphragm is retroperitoneal and supports all the viscera. Composed of the: Levator ani group: puborectalis, pubococcygeus, and ileococcygeus. Coccygeous muscles Question #1 In a CT scan of the pelvis, the uterus is located: A) Posterior to the bladder and rectum B) Posterior to the bladder and anterior to rectum C) Anterior to the bladder and rectum D) Anterior to the bladder and posterior to the rectum Answer B) Posterior to the bladder and anterior to the rectum. Question #2 A 27 year-old woman is examined by her gynecologist. Upon rectal examination, a firm structure, directly in front of the rectum, in the midline, is palpated through the anterior wall of the rectum. The structure is: A) Bladder B) Body of uterus C) Cervix of uterus D) Pubic symphysis E) Vagina Answer C) Cervix of uterus The cervix of the uterus is anterior to the rectum Since the cervix is the inferior part of the uterus that is protruding into the vagina, it should feel like a firm structure upon palpation Although the vagina is directly anterior to the rectum, it would not feel like a distinct and firm structure upon palpation.