Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
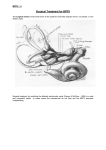
B.P.P.V. & Vestibular neuronitis Dr. Vishal Sharma Benign Paroxysmal Positional Vertigo Introduction Most common cause of vertigo arising from peripheral labyrinthine dysfunction 20% of vertigo cases in all age groups 50% of vertigo cases in elderly pt Average age of onset: 50-60 years Male : female = 2:1 Etiology Idiopathic (50% of all cases) Head injury (pt < 50 yrs) Vestibular degeneration (pt > 50 yrs) Viral labyrinthitis Otitis media Meniere’s disease Following ear surgery Prolonged bed rest Pathogenesis POSTR S.C.C. CUPULA UTRICLE MACULA Pathogenesis Otoconial debris (calcium carbonate) released from degenerating macula of adjacent utricle floats freely in endolymph settles on cupula of posterior semicircular canal in a critical head position causes displacement of cupula & vertigo Types of BPPV Posterior semicircular canal BPPV: 80 - 85 % Lateral semicircular canal BPPV: 15 - 17 % Superior semicircular canal BPPV: < 5 % Lateral & superior semicircular canal BPPV mostly caused by faulty treatment maneuvers of posterior semicircular canal BPPV Symptoms 95% cases have unilateral BPPV Vertigo in a certain head position Inability to roll in bed or to look up high Nausea & vomiting in severe conditions There is no hearing loss Absence of other neurologic symptoms Nystagmus in B.P.P.V. Duration: < 1 minute due to adaptation Asthenia (fatiguing): on repeating maneuver Latent period: of 2–20 sec before nystagmus Direction: fixed, rotatory, geotropic & reverses on return to sitting position Associated symptoms: vertigo, vomiting, excessive sweating Management of B.P.P.V. Diagnosis: Dix-Hallpike positional maneuver Treatment: Epley’s canalith repositioning maneuver Semont’s liberatory maneuver Home exercises Surgical treatment Diagnosis Dix-Hallpike test is diagnostic for posterior semicircular canal BPPV Dix-Hallpike test done with Frenzel’s glasses & video display gives better accuracy Electro-nystagmography does not record rotatory component of nystagmus Other investigations not required for diagnosis Frenzel glasses Dix – Hallpike maneuver (Nylen – Barany maneuver) Step 1 (for Right ear) 3 Step 2 Step 3 Step 4 Steps 1 to 3 Step 3 to 4 Dix-Hallpike Maneuver 1. Pt in sitting position on a couch looking ahead 2. Pt’s head turned 45° towards diseased ear 3. Pt moved rapidly into supine position with head hanging 30° below couch. Pt’s eyes observed for nystagmus for 1 minute 4. Pt moved rapidly back into sitting position 5. Maneuver repeated for opposite ear Epley’s particle repositioning maneuver for right ear Step 1 3 Step 2 Step 3 Step 4 Step 5 Step 6 Step 5 to 6 Step 7 Epley’s Maneuver for Rt ear 1. Pt in sitting position on a couch looking ahead 2. Pt’s head turned 45° towards diseased ear 3. Pt moved rapidly into supine position with head hanging 30° below couch 4. Pt’s head rotated by 90° to opposite side 5. Further 90° head + trunk rotation Epley’s Maneuver for Rt ear 6. Pt moved rapidly back into sitting position & pt’s head brought in midline 7. Slight flexion of pt’s head Cervical collar given to pt for 48 hours Pt must have nystagmus at every step of Epley’s manoeuvre if it is done properly 80% pt get cured by a single maneuver Advice after maneuver Wait for 30 minutes before going home Do not drive yourself home Home advice Avoid violent head jerks & head positions that trigger positional vertigo for at least 1 week Sleep in 45o head end elevation for 48 hr. 1 week after tx, carefully put yourself in position that usually makes you dizzy. Let your doctor know how you felt. If Epley’s maneuver fails Repeat Epley’s maneuver after 1 month Try Semont’s maneuver Advice home exercises If all maneuvers & exercises fail, diagnosis is clear & symptoms are intolerable: Surgical Therapy Semont’s maneuver for Rt posterior canal BPPV 1. Sit upright with head turned 45° toward left 2. Drop quickly to right by 900. Debris moves towards apex of posterior SCC. Wait for 30 sec after nystagmus stops. 3. Move head & trunk swiftly toward left by 1800 Debris moves towards exit of posterior SCC. Wait again for 30 sec after nystagmus stops. 4. Sit upright again. Debris falls into utricle. 5. Performed 3 times a day for 2 weeks Home Exercises 1. Brandt-Daroff Exercise 2. Home Epley’s Maneuver Indications: Diagnosis is clear & patient well-trained Absence of other causes of vertigo Pt must report immediately if neurological symptoms appear during exercise due to vertebral artery compression Home Epley’s maneuver Brandt-Daroff Exercise 1. Sit upright. 2. Drop quickly to right by 900, with head angled upward by 450. Stay for 30 seconds. 3. Sit upright again. Stay for 30 seconds. 4. Drop quickly to left by 900, with head angled upward by 450. Stay for 30 seconds. 5. Sit upright again. Perform 5 sets, thrice / day for 2 weeks. Surgical treatment Considered when Epley maneuver, Semont maneuver + Brandt-Daroff exercises have failed and diagnosis of BPPV is clear 1. Posterior semicircular canal plugging (Parnes) 2. Singular neurectomy (Gacek) Posterior SCC plugging Gacek’s singular neurectomy Atypical BPPV Lateral Canal BPPV: debris in lateral SCC Superior Canal BPPV: debris in superior SCC Cupulo-lithiasis: Debris stuck to canal side of semicircular canal cupula Vestibulo-lithiasis: Loose debris present on vestibule-side of semicircular canal cupula Multi-canal BPPV: debris in multiple SCC Etiology of atypical BPPV Nystagmus (fast component) Semicircular canal stimulated Nystagmus Direction Right Lateral Right horizontal Left Lateral Left horizontal Right Superior Down beating, counter-clockwise Left Superior Down beating, clockwise Right Posterior Up beating, counter-clockwise Left Posterior Up beating, clockwise Diagnosis: Lateral canal BPPV: Roll test horizontal nystagmus towards lower ear Superior canal BPPV: Dix Hallpike test torsional ageotropic nystagmus Treatment: Lateral canal BPPV: 3600 contralateral Roll test, canal plugging in failure cases Superior canal BPPV: Epley’s maneuver of opposite side, canal plugging Posterior SCC BPPV Superior SCC BPPV Up-beating, torsional nystagmus Down-beating, torsional nystagmus Geotropic (superior pole moves towards lower ear) during Dix-Hallpike maneuver Ageotropic (superior pole moves towards upper ear) during DixHallpike maneuver *** *** during Dix Hallpike maneuver, opposite (upper) superior SCC gets stimulated & its clock wise movement becomes ageotropic nystagmus Roll Test for lateral canal BPPV 1 2 3 4 5 Roll test for lateral canal BPPV 1. Patient lies supine with nose pointing up 2. Head turned 900 right rapidly & kept for 30 sec 3. Head turned back to supine position for 30 sec 4. Head turned 900 left rapidly & kept for 30 sec 5. Head turned back to supine position for 30 sec Watch for nystagmus after each step 0 360 contra-lateral Roll over maneuver for left lateral canal BPPV 1 2 3 4 5 1. Patient lies supine with nose pointing up 2. Head turned 900 into Rt lateral decubitus 3. Head turned further 900 into prone position 4. Head turned further 900 into Lt lateral decubitus 5. Head turned further 900 into supine position Each position kept for 30 sec & watch for nystagmus Vestibular neuronitis Clinical presentation Occurs most commonly in middle-aged adults Acute, sustained peripheral vestibular dysfunction with nausea, vomiting, severe vertigo & imbalance Preceded by upper respiratory tract infection After 24 hours of onset, vertigo intensity decreases progressively & most patients recover from severe vertigo & imbalance within 1-3 weeks Third most common cause of peripheral vertigo after BPPV & Meniere’s disease Etiology: Viral infection of vestibular nerve Acute localized ischemia of vestibular nerve Auto-immune injury of vestibular nerve Recurrence of symptoms due to dormant Herpes virus in Scarpa’s vestibular ganglion Presence of Spontaneous, unidirectional, Absence of Direction changing nystagmus horizontal, nystagmus beating Hearing loss towards healthy ear, Other cranial nerve deficits suppressed by optic fixation Brain-stem & Cerebellar signs Rhomberg test: fall towards Middle ear infection diseased side High fever Caloric test: I/L canal paresis Neck rigidity Treatment of Acute attack Reassurance Bed rest + head support Inj. Prochlorperazine (Stemetil): 12.5 mg I.V., T.I.D. – Q.I.D. Inj. Promethazine (Phenergan): 25 mg I.V., T.I.D. – Q.I.D. Inj. Diazepam (Calmpose): 5 mg I.V. stat Subsequent Treatment Oral Cinnarizine: 25 mg TID to 75 mg BD for 7 days Oral Betahistine: 16 mg TID for 2 - 4 weeks 3-week course of methyl prednisolone tapered from 100 mg down to 10 mg daily may reduce long- term loss of vestibular function Anti-viral drugs have no benefit Thank You