Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
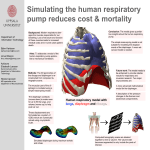
Respiratory Physiology Respiration: General • Purpose- To stay alive • Speech is an overlaid function • Respiratory patterns different for: – Breathing for life – Breathing for speech Relationship of Lung, Thorax & Abdomen • Motion of rib cage & diaphragm cause volume change (inc. & dec) • Surface of lungs linked to surface of thoracic walls & diaphragm – Linkage- Fluid interface between pleura • Visceral Pleurae- lines lung • Parietal Pleurae- lines thoracic cavity • Pleural cavity- space between visceral & parietal linings • Thoracic & diaphragm movement cause LV inc. & dec. – Inhalation: Lung volume and pressure Pleural Linkage • Function of surface tension of the fluid in pleural space – e.g.. Wet sheets of glass (resist separation but free to move) • Only surface tension accounting for pleural linkage? No, linkage a function of: – Fluid transport out of pleural space – Elasticity of pleura itself Linkage: Diaphragm & Rib Cage • Diaphragm attaches to inferior rib cage – rib cage expands = increase in diaphragm circumference – contraction of diaphragm elevates lower rib cage (Superior fibers & costal attachment) – Rib cage & diaphragm not independent Linkage: Diaphragm & Abdomen • Linked via interposed abdominal viscera – abdominal cavity bound by 2 moveable walls • Diaphragm above • Muscular abdominal walls anterior and lateral • Lowering diaphragm increases abdominal pressure – Drives abdominal wall out Intrapleural Pressure Insp Larynx Trachea Exp Alveolar Pressure Pressure (cm H2O) Intrapleural Pressure Lungs Visceral Pleura Parietal Pleura Volume (Liters) Lung Volume Time (Seconds) Percent Vital Capacity Respiratory Volumes Inspiratory Volume Reserve Vital Capacity Total Capacity Tidal Volume Expiratory Volume Reserve Residual Residual Volume Volume Tidal Volume Resting Expiratory Level Functional Residual Capacity Inspiratory Reserve Volume Vital Capacity Total Lung Capacity Inspiratory Capacity Tidal Volume (Increasing Activity) Expiratory Reserve Volume Residual Volume Spirometer for measuring respiratory volume Measurement of Respiration • Respiratory flow, volumes & capacities are measured using a spirometer Amount of water displaced gives you estimate of the air required to displaces it Recording Drum Air Chamber Water Measurement of Respiration Manometer -Measures Pressure; more force used the higher the water rises cm H2O Respiration for Life • Quiet respiration & Forced respiration – Economy of effort – Minimum departure from the resting volume – Relaxed balance exists between tendencies of thorax expansion & lung collapse – Balance is typically at 35-40% of vital capacity (amount available for use) – Quiet inspiration= the volume of air that can be inhaled from a resting level with muscle contraction – Quiet expiration= Passive process by elastic recoil of lungs & abdomen Quiet Respiration Insp. Exp. Percent of Vital Capacity 40% 60% 40 Resting Volume 0 Resting Tidal Volume *Volume of air move called resting tidal volume *40% of cycle spent on inspiration; 60% of cycle spent on expiration Forced Respiration • Increased energy demands for air exchange in lungs – muscular support recruited for insp. & exp. – Forced insp.= ? – Forced expiration=? • Go beyond resting inhalation or exhalation= recruit muscle involvement • Time spent about the same as in quiet respiration Respiration for Life • Ventilation – Actual movement of air in the conducting respiratory pathway – Air distributed: 3 million alveoi; perfused (picks up oxygen) through 6 million capillaries – Diffussion takes place (actual gas exchange across alveolar-capillary membrane) Development • Developmental Changes (infancy-adulthood): – Increase in VC – VC increases fairly regularly with age – Young adult 3.5-5 times the lung volume of a 5 year old child – VC depends on volume of lung tissue – Peak reached in late teens or 20’s – Decrease after early 20’s & reduction of diaphragmatic action – Residual volume increase with age Vital Capacity Based on Age & Gender VC (ml) Male Female Age (Years) Typical Respiratory Volumes & Capacities in Adults Volume/ Capacity VC Resting TV TLC Females (cc) Males (cc) Average (in cc) 3200 cc 4800 cc 4000 cc 450cc 600 cc 525cc 4800 cc 6000 cc 5100 cc Females: VC in ml= 21.78- (0.101 x age in years) x ht.in cm Males: VC in ml= 27.63- (0.112 x age in years) x ht.in cm Breathing for Speech • Same respiratory equipment and measures of air volume &lung capacity apply for speech breathing • Difference? How & Why they are used! – Life- Objective to move O2 & CO2 in & out of lungs • resistance interferes – Speech- Objective to have air under pressure; force vocal folds to vibrate • Achieve pressure by resisting airflow Respiratory Pressures • Alveolar Pressure • Intrapleural Pressure • Subglottal Pressure • Intraoral Pressure • Atmospheric Pressure Respiratory Pressures Atmospheric Intraoral Subglottal Intrapleural Respiratory Pressures • Atmospheric (Patm): Exerts pressure on earth’s surface; our reference with which to compare resp. pressures (zero) • Intraoral (Pm): Pressure within the mouth • Subglottal (Ps): Pressure below the vocal folds • Intrapleural (Ppl): Pressure in the space between the parietal and visceral pleura Reading • Readings: – Seikel: Ch. 4, (Pgs.121-142) – Maue-Dickson: Ch.3 (Pgs. 81-87)