Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Peripheral Nervous System (PNS)
1
Nervous System Classification-1
• Somatic Nervous System
– Motor nerves to skeletal muscle (somatic motor neurons)
• Upper and lower motor neurons
– Skeletal Muscle Reflexes
• Sensory, interneurons, lower motor neurons
– Visceral (organ) Reflexes
– Sensory nerves (somatosensory neurons)
• Autonomic Nervous System
– Motor nerves to smooth and cardiac muscle (visceral
motor neurons)
Today’s lectures
• Sympathetic
are the red topics
• Parasympathetic
2
Nervous System Classification-2
• Efferent Nervous System
• Somatic Nervous System
•
Upper and lower motor neurons to skeletal
muscle (somatic motor neurons)
• Visceral (Autonomic) Nervous System
– Motor nerves to smooth and cardiac muscle (visceral
motor neurons)
I did not organize the
• Sympathetic
lectures by this method
• Parasympathetic
of classification
• Afferent Nervous System
• Sensory nerves (somatosensory neurons)
• Reflexes
3
VISCERAL (“organ”)
MOTOR NERVES
• A visceral motor nerve innervates involuntary
effectors (smooth muscles in organs). This is
part of the ANS.
• A somatic motor nerve innervates voluntary
effectors (skeletal muscle). It is not part of the
ANS.
– (don’t confuse this with a somatic sensory nerve for
the sense of touch; sensory nerves are not part of the
ANS either)
4
VISCERAL (“organ”) SENSES
• Internal organs also have sensory nerves that
tell you when you have eaten enough or your
bladder is full. These are not part of the ANS
because they are sensory.
• Not all organs have sensory nerves, for
instance, you can’t feel when you have high
blood pressure.
• You can also have visceral reflexes, which
trigger the parasympathetic system to contract
the bladder when full, etc.
• Reflexes are hard to localize.
5
Nervous System Classification-1
• Somatic Nervous System
– Motor nerves to skeletal muscle (somatic motor neurons)
• Upper and lower motor neurons
– Skeletal Muscle Reflexes
• Sensory, interneurons, lower motor neurons
– Visceral (organ) Reflexes
– Sensory nerves (somatosensory neurons)
• Autonomic Nervous System
– Motor nerves to smooth and cardiac muscle (visceral
motor neurons)
• Sympathetic
• Parasympathetic
6
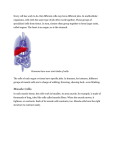
Somatosensory Neurons
• The somatosensory system is made up of a number of
different neurons with various receptors, including
thermoreceptors (action potential is triggered by heat or
cold), photoreceptors (triggered by light),
mechanoreceptors (triggered by movement) and
chemoreceptors (triggered by chemicals), proprioception
(position of the body), and nociception (pain).
• Each somatosensory neuron specializes in conducting
one type of sensation.
• The sensory receptors cover the skin, skeletal muscles,
bones and joints, internal organs, and the cardiovascular
system.
7
Somatic Senses
• Pain
• Haptic perception
– Deep Pressure
– Light Touch
•
•
•
•
•
These are routinely tested
by doctors in a physical
exam, especially for
people with diabetes and
lupus.
Vibration
Thermoception (Hot/Cold)
Two-point discrimination
Proprioception
Special senses
8
Sense of Touch
• “Touch” is a layman’s term. It is not
specific in what it describes.
• Touch includes mechanoreception (deep
pressure, light touch, vibration and
proprioception), pain (nociception) and
heat (thermoception).
9
Sense of Pain
• A nociceptor is a receptor of a sensory
neuron (nerve cell) that responds to
potentially damaging stimuli by sending
signals to the spinal cord and brain.
• This process, called nociception, usually
causes the perception of pain.
• They travel in the dorsal column pathway
in the spinal cord, ascend to the thalamus
in the brain, and go to the cerebral cortex.
10
Referred Pain
• Pain in an organ may not be where the organ is.
• Heart pain usually manifests in the left side of
chest, the left shoulder, arm, but not the heart.
• This is REFERRED PAIN.
• Pain in the lungs usually shows up as neck pain.
• These areas of referred pain are important to
know, but not for this class.
11
A Map of Referred Pain
12
Complex regional pain
syndrome (CRPS)
• Formerly called Reflex Sympathetic Dystrophy (RSD)
• Chronic progressive disease characterized by severe pain, swelling,
and changes in the skin.
• It often affects an arm or a leg and may spread to another part of the
body and is associated with dysregulation of the autonomic nervous
system resulting in multiple functional loss, impairment, and
disability.
• Symptoms include burning and shooting pains and edema that
occur more often during times of stress.
• Treatment is often unsatisfactory. Early multimodal therapy can
cause dramatic improvement or remission of the syndrome in some
patients.
• http://losangeles.cbslocal.com/video/9805202-theres-no-cure-forcomplex-regional-pain-syndrome-but-doctors-say-treatment-offers- 13
hope/
Treatment for Pain
• Somatosensory Rehabilitation of Pain is a
method whose aim is to treat conditions of
a reduced sense of touch or sensation
(hypoesthesia) in order to decrease
neuropathic pain.
• Neuropathic pain, with a prevalence of
6.9% of the general population, represents
an important public health problem.
14
Treatment for Pain
• Examples of pain syndromes include:
• Carpal Tunnel Syndrome (CTS) concerns
2.7% of the general population.
• Complex Regional Pain Syndrome
(CRPS) concerns 26/100,000.
• Patients with chronic pain might use
transcutaneous electrical nerve stimulation
(TENS unit) and other physical therapy
modalities, which bring substantial pain
15
relief to large numbers of people.
Haptic perception
(Sense of Touch)
–Deep Pressure
–Light Touch
16
• While touch (also called tactile perception) is
considered one of the five traditional senses,
the impression of touch is formed from
several modalities including pressure, skin
stretch, vibration and temperature.
• There are separate neurons for each of
those sensations, and each group of
neurons must be evaluated during a physical
exam.
• In medicine, the colloquial term "touch" is
usually replaced with "somatic senses" to
better reflect the variety of mechanisms
17
involved.
Haptic perception
• Haptic perception is the process of
recognizing objects through touch. It
involves a combination of somatosensory
perception of patterns on the skin surface
(e.g., edges, curvature, and texture) and
proprioception of hand position and
conformation (what position do my finger
go into while tracing the surface of the
object?).
18
Haptic perception
• People can rapidly and accurately identify
three-dimensional objects by touch.They
do so through the use of exploratory
procedures, such as moving the fingers
over the outer surface of the object or
holding the entire object in the hand.
19
• Haptic perception is active exploration,
whether with a body part or a tool, such as
feeling the contours of something by using
a stick to touch it.
• Haptic perception allows the creation of
"virtual", illusory haptic shapes with
different perceived qualities.
• Loss of the sense of touch is a
catastrophic deficit that can impair walking
and other skilled actions such as holding
objects or using tools.
20
Disorder of Sense of Touch
• One disorder of the sense of touch:
• Allochiria
21
Allochiria
• Allochiria (from the Greek meaning "other hand") is a
neurological disorder in which the patient responds to
stimuli presented to one side of their body as if the
stimuli had been presented at the opposite side.
• It is associated with spatial transpositions, usually
symmetrical, of stimuli from one side of the body (or of
the space) to the opposite one. Thus a touch to the left
arm will be reported as a touch to the right arm
• If the auditory or visual senses are affected, sounds (a
person's voice for instance) will be reported as being
heard on the opposite side to that on which they occur
and objects presented visually will be reported as having
been presented on the opposite side.
22
• Commonly from damage to the right parietal lobe.
Allochiria
Allochiria can also occur to other senses.
• Motor Allochiria
• Reflex Allochiria
• Audio Allochiria
• Visual Allochiria
• Gustatory Allochiria
23
Sense of Vibration
• Pallesthesia refers to the sensation of
mechanical vibration on or near the body.
• Vibration sense may be lost as a result of a
number of lesions to the nervous system, often
in conjunction with other deficits.
• The word "pallesthesia" is derived from the
Greek pallein, meaning "to shake."
• Pallesthesia may be tested for using a vibrating
mechanical tuning fork, placed on a bony
prominence.
24
Thermoception
(Sense of Hot/Cold)
• Thermoception is the sense of heat and the absence of
heat (cold) by the skin.
• There are specialized receptors for cold (declining
temperature) and for heat.
• Cold receptors help an animal’s sense of smell, telling
wind direction. Heat receptors help animals that can use
radiation to detect prey, such as snakes.
• The information travels up the spinothalamic tract in the
spinal cord and ascends to the thalamus.
• The thermoceptors in the skin are quite different from the
homeostatic thermoceptors in the brain (hypothalamus),
which provide feedback on internal body temperature.
25
Two-point discrimination
• Two-point discrimination is the ability to
discern that two nearby objects touching
the skin are truly two distinct points, not
one.
• It is often tested with two sharp points
during a neurological examination and is
assumed to reflect how finely innervated
an area of skin is and diagnosing tactile
agnosia (don’t know what is touching me).
26
Two-point discrimination
• The therapist randomly alternates between
touching the patient with one point or with
two points on the area being tested (e.g.
finger, arm, leg, toe).
• The patient is asked to report whether one
or two points was felt. The smallest
distance between two points that still
results in the perception of two distinct
stimuli is recorded as the patient's two27
point threshold.
Two-point discrimination
• Performance on the two extremities can
be compared for discrepancies.
28
PROPRIOCEPTION
• There are sensors within the muscles and joints that
measure the amount of force, movement, and position.
• Proprioception neurons travel up the spinocerebellar
tract. The brain can then interpret whether you are off
balance, then send a command to the muscles to
contract and straighten yourself up so you don’t fall.
• Note that this sense of balance is NOT the same as the
sense of balance from equilibrium in the ears.
Proprioception neurons are located within the muscles
and joints.
• During a physical exam, a doctor will test the patient’s
proprioception ability by telling them to close their eyes
and place their finger on their nose. This may indicate a
lesion in the cerebellum. Who else may ask you to do
29
this test? Alcohol disrupts the cerebellum.
Muscle spindles
• Muscle spindles are sensory receptors
within the belly of a muscle that primarily
detect changes in the length of this
muscle. The brain can then determine the
position of body parts.
• Muscle spindle responses also play an
important role in regulating the contraction
of muscles, by activating motor neurons
via the stretch reflex to resist muscle
stretch.
30
Proprioceptors
•Sensory receptors
that report on
internal events in
your muscles and
joints.
•They report on
muscle stretch and
joint position.
•They generate
electrical impulses
that will travel up
neurons to the
CNS.
•A muscle spindle is
one type of
proprioceptor.
31
Proprioception Disorders
• Not enough vitamin B1 (memory problems)
• Too much vitamin B6 (balance problems)
– Damage to proprioceptors can occur from consuming
excess vitamin B6 (pyridoxine).
– Patients cannot tell where their body parts are unless
they look at them.
– They have difficulty with all motor tasks including
walking, eating, dressing, etc.
– They must use their vision to watch each body part to
make it move in the right direction.
32
PROPRIOCEPTORS
• Proprioception is often tested by having the patient
close their eyes and saying if their fingers are up or
down.
• Proprioceptors send information to the cerebellum. That’s
how you know your legs are crossed before you stand up.
• Somatic senses and proprioception are NOT
considered special senses.
33
Special senses
• The special senses are those that have
specialized organs devoted to them:
• vision (the eye)
• hearing and balance (the ear)
• smell (the nose)
• taste (the tongue)
These will be discussed in
a separate lecture.
34
• Somatic sense information goes into the
spinal cord, travels up a tract and into the
primary somatosensory area in the parietal
lobe of the cerebral cortex.
• The mapping of the body surfaces in the
brain is called a homunculus and plays a
fundamental role in the creation of body
image.
This brain-surface ("cortical")
map is not immutable, however.
Dramatic shifts can occur in
response to stroke or injury.
35
SENSORY CUTANEOUS
NERVES
• These come out of the spinal cord and go
to specific regions of skin on the body.
• For example, nerve C4 innervates the skin
region C4 of the DERMATOME MAP.
• It’s important to know these dermatome
map regions (not for this class), especially
physical therapists and nurses.
36
Dermatome Map
•
•
•
If a patient has a shooting pain
down the anterior shin, what
nerve is pinched? L5.
Numbness in pinky and ring
finger is what nerve? C8.
If a workman’s comp patient
comes in saying his whole
hand is numb, no other
symptoms, you know he’s lying
because the nerves don’t run
that way.
37
DAMAGE TO THE
NERVOUS SYSTEM
• If a person has a spinal cord injury in their
cervical region, they could have
quadriplegia/tetraplegia (arms and legs
paralyzed).
• If a person has a spinal cord injury in their
thoracic region, they could have
paraplegia (just legs are paralyzed).
38
Disruption of Blood Supply
• When a body part “falls asleep”, the region
has become ischemic (lack of blood flow),
impairing the action potential of the
nerves.
• Unlike the CNS, when blood is restored to
the PNS, the nerves recover.
• Damage to the CNS tends to be
permanent, but damage to the PNS tends
to heal.
39
Cut nerves
• If a small nerve is cut, it will regenerate
because where are the cell bodies? In the
posterior root ganglion (sensory) or
anterior horn (motor).
• Since the cell body is about a meter away,
axons can regrow.
• Large nerves are harder to regrow, but
you can still stitch the ends together at the
epineurium and perineurium, and you may
get healing.
40
Doctors trying to fix damaged nerves
•
http://www.foxnews.com/health/2012/11/13/doctors-trying-to-fix-damaged-nerves/
• Nerve disease and injuries are tough to treat, largely
because there's no way to regenerate many damaged
nerve cells. Neurologist Joseph Corey is trying to change
that.
• Corey and a team of scientists used tiny polymer fibers
as a scaffold. They coaxed an oligodendrocyte to form a
myelin sheath around the fiber. The artificial fiber
mimicked an axon.
• Myelin provides the pathways along which some nerve
cells regenerate after an injury. When a person has MS
or cerebral palsy, the oligodendrocytes are damaged and
don't function properly and the myelin sheaths start to
break down.
41
Rat Brain in a Dish Flies Plane
• An electrode grid was
placed at the bottom of a
glass dish and then
covered with rat neurons
that gradually formed a
neural network -- a brain.
• They then used the brain
to control an F-22 fighter
jet flight simulator.
• The research could lead to
tiny, brain-controlled
prosthetic devices and
unmanned airplanes flown
by living computers.
42
Exoskeleton Helps Paralyzed Patients Walk
•
•
Exoskeletons have been
designed for military use and
boosting strength. But the same
technology that makes people
able to lift heavier loads might
also one day allow those with
spinal injuries to walk.
Ekso Bionics, a California
company, developed the Human
Universal Load Carrier, or HULC
for the military, and another one
called the Ekso, for people who
need either physical therapy or
rehabilitation.
43
Tens unit
• Transcutaneous electrical nerve
stimulation
TENS is usually applied at high
frequency with an intensity below
motor contraction. It just blocks
pain impulses.
This is a different machine than a
muscle stimulator, but they look the
same.
TENS is available without a Rx.
44
Corydalis powder for pain
•
http://www.prevention.com/health/health-concerns/chinese-remedy-corydalis-pain
Put ½ teaspoon into one cup of hot
fluid (tea, etc) and drink it.
Alleviates chronic pain in about 20
minutes!
45
Pinched nerves
• When a nerve gets pinched (e.g. herniated
disc), it damages the nerve by interfering
with its action potential, causing
weakness, pain, or paralysis.
46
Spinal Nerves Posterior View
47
SOME CLINICALLY IMPORTANT
PERIPHERAL NERVES:
• Note: an epidural nerve block during child birth
will numb the mother from her navel to her
knees.
• PUDENDAL NERVE: this is the nerve that can
be anesthetized during childbirth as an
alternative to an epidural (a pudendal nerve
block is also called a saddle block because the
numb areas are where you would be touching a
saddle).
• PHRENIC NERVE: allows the diaphragm to
contract. If it gets severed, the person can no
48
longer breathe without assistance.
Nerve Plexus
A PLEXUS is a network of nerves that
primarily serves the limbs. There are four
major plexi: cervical, brachial, lumbar, and
sacral.
1. CERVICAL PLEXUS comes out of the
neck and are cutaneous nerves (sensory
input of the skin) of the neck and back of
the head. The phrenic nerve (supplies the
diaphragm) is also in this plexus.
49
Cervical
Plexus
50
BRACHIAL PLEXUS
2. BRACHIAL PLEXUS
• This is the major group of nerves that supply the
upper limbs. It runs through the axilla.
• If a person leans their armpits on their crutches,
they can damage this plexus and lose the use of
their arms.
• The nerves in the brachial plexus change names
as they go to different regions in the arm.
51
The Brachial Plexus
52
Axillary
Musculocutaneus
Major Nerves
of the Upper
Extremity
53
Axillary Nerve
• Deltoid
54
Musculocutaneus
Nerve
• Supplies anterior
muscles of the arm
55
Instead of radial and ulnar nerve, we have median and ulnar nerve.
Median Nerve
• Supplies no muscles of the arm
• Supplies anterior forearm (except flexor
carpi ulnaris)
• Damage can cause
– Hand of benediction
– Ape Hand
– Carpal Tunnel Syndrome
Patient trying to
make a fist
56
MEDIAN NERVE: Ape Hand
• This is the nerve that gets cut when people try to
slit their wrists.
• The arteries are so small in the wrist; people
rarely die from this type of suicide attempt.
• However, they live with a lot of tissue damage.
• They are not able to move the thumb towards
the little finger, so it is hard to pick up small
objects.
• This is called “ape hand”.
57
58
Carpel Tunnel Syndrome
59
Median Nerve:
Carpel Tunnel Syndrome
• The median nerve
travels under the
transverse carpal
ligament.
• The nerve is
pinched in carpal
tunnel syndrome.
60
Carpel Tunnel Syndrome
61
Patient Case
• George has been a computer programmer
for 20 years. He has numbness in his right
hand on the thumb, index finger, and
middle finger.
• Tapping on the carpal tunnel causes
parathesias (tingling) in the median nerve
distribution (positive Tinel’s sign).
• Placing his wrist in sustain flexion for one
minute also causes the parathesias
62
(positive Phalen’s test).
Patient Case
• Treatment began with splinting the wrist in
neutral position and patient education for
proper ergonomics (how to use your body
at work without injury). George was told to
use a wrist pad while typing).
63
Trigger Finger
• Trigger finger is one example of the
disability that can be created when
repetitive trauma to a flexor tendon results
in the formation of nodules on the tendon.
Finger flexion may be prevented
completely, or the finger may be unable to
re-extend.
64
Ulnar Nerve
• Supplies flexor carpi ulnaris
• “Funny Bone”
• Damage can cause claw hand; cannot
adduct or abduct fingers
65
Radial Nerve
• Supplies muscles on the posterior arm and
forearm
– Triceps brachii
– Extensor carpi radialis
– Extensor digitorum communis
• Damage can cause wrist drop
• Also called “waiter’s hand”
66
Carpel Tunnel Syndrome
Ape Hand
67
Axillary,
Musculocutaneus,
Ulnar, Median,
Radial, Nerves
68
Figure 14.4
Brachial Plexus
• Damage to Brachial Plexus
– Congenital (brachial plexus damaged during birth;
the baby comes out arm first and someone pulls it)
• Klumpke’s paralysis
– Acquired Brachial Plexus injuries
• Crutch paralysis (total upper extremity paralysis)
• Claw Hand
• Carpal Tunnel Syndrome, Ape hand, Hand of
benediction
• Wrist Drop (Waiter’s Hand)
69
LUMBAR PLEXUS
3. LUMBAR PLEXUS
• FEMORAL NERVE is the main nerve to
the anterior thigh.
70
Lumbo-Sacral Plexus
• Lumbar:
– Femoral nerve
• Sacral:
– Sciatic nerve
71
The Lumbar Plexus
72
Figure 14.15
Sacral Plexus
4. SACRAL PLEXUS are spinal nerves from L4-S5
• Some of the fibers from the lumbar plexus mix with the
sacral plexus, so these are often referred to together as
the lumbosacral plexus.
• SCIATIC NERVE is the largest branch of the sacral
plexus and the largest nerve in the body; it is about the
size of your pinky finger. It leaves the pelvis through the
greater sciatic notch.
• A short, thick muscle (Piriformis muscle) covers the
greater sciatic notch, and when it contracts, it can pinch
the sciatic nerve, causing a type of sciatica (sciatic nerve
irritation) known as piriformis syndrome.
• This can be alleviated by stretching exercises (lay on
back and move knee to opposite shoulder). However,
sciatica can also be caused if there is a herniated lumbar
disc, in which case stretching exercises make it worse.
73
The Sacral Plexus
74
Figure 14.16a, c
75
• Sciatica tremors video
76
Spinal steroid shots may have little
effect on sciatica
•
http://www.foxnews.com/health/2012/11/13/spinal-steroid-shots-may-have-little-effect-on-sciatica/
• For the back pain component of sciatica, the researchers
found that the injections didn't seem to make a difference
over short or long periods of time.
• When it came to leg pain, there was no difference a year
or so after the injection, but there was a statistically
significant drop in pain scores over the short term - about
2 weeks to 3 months.
77
78
Obturator
Femoral
Nerves of the
Lower
Extremity
The sciatic nerve supplies
the back of the thigh, then
branches out into the
TIBIAL and FIBULAR
(peroneal) nerves, which
supply the leg and foot.
The fibular nerve
branches into superficial
and deep.
79
Lower Extremity Nerves
Obturator Nerve
Supplies adductor muscles
Femoral Nerve
Supplies anterior Thigh
Sciatic Nerve
Supplies posterior thigh
Tibial Nerve
Supplies posterior leg and foot
Common Fibular Nerve
Superficial branch
Supplies lateral side of leg
Deep branch
Supplies anterior leg
Injury causes “Foot Drop”
80
Tibial Nerve
• Sometimes a small branch of the tibial nerve in
the foot gets pinched between the metatarsal
heads, and the irritation causes nerve swelling
and pain.
• It is called a neuroma (“nerve tumor”) and
manifests as pain in the ball of the foot, made
worse with high heels.
81
82
Nervous System Classification-1
• Somatic Nervous System
– Motor nerves to skeletal muscle (somatic motor neurons)
• Upper and lower motor neurons
– Skeletal Muscle Reflexes
• Sensory, interneurons, lower motor neurons
– Visceral (organ) Reflexes
– Sensory nerves (somatosensory neurons)
• Autonomic Nervous System
– Motor nerves to smooth and cardiac muscle (visceral
motor neurons)
• Sympathetic
• Parasympathetic
83
Efferent Nervous System
Somatic
Division
Skeletal muscle
Visceral
(Autonomic)
Division
Parasympathetic
Sympathetic
Blood vessel
Adrenal
Gland
Smooth muscle,
cardiac muscle,
and glands
AUTONOMIC NERVOUS SYSTEM
• We don’t have voluntary control over these
nerves.
• They are involved digestion, blood flow,
urination, defecation, glandular secretion.
• Therefore, the ANS supplies the glands,
smooth muscle, and cardiac muscle, but
NOT the skeletal muscle.
• For this reason, the ANS is also called the
general visceral motor system.
85
Sympathetic Division of the ANS
86
ANS
• All of the neurons of the ANS are motor neurons
(there are no sensory neurons in the ANS).
• The ANS motor neurons differ from the somatic
motor neurons (for skeletal muscle) because the
ANS has two lower motor neurons in the
periphery (the cell body of one is in the spinal
cord and the cell body of the other is in the
periphery), whereas the somatic motor neurons
have one lower motor neuron, and its cell body
is within the spinal cord, not in the periphery.
87
ANS has TWO lower motor neurons
Preganglionic
neuron
Somatic system has just
one lower motor neuron
Post-ganglionic
neuron
Ganglion (where the cell
bodies of the postganglionic neurons are)
88
ANS
• The ANS lower motor neuron comes from the
spinal cord and synapses on the cell body of
another neuron, which then synapses on the
target (gland, blood vessel or organ).
89
Ganglia
• The area where the two neurons come together is the
AUTONOMIC GANGLIA.
• The first neuron is the PRE-GANGLIONIC NEURON.
• The second neuron is the POST-GANGLIONIC NEURON.
90
ANS
• The ANS motor unit is characterized by
having more than one lower motor neuron,
the axons are usually unmyelinated (since
they are only going to organs), conduction
is slow, and the axons are thin (which also
slows conduction like a freeway with only
one lane).
• The ANS has two divisions: sympathetic
and parasympathetic.
91
SYMPATHETIC DIVISION
(has nothing to do with sympathy!)
• ↑heart rate and blood pressure,
• ↑metabolic activity (increased blood
glucose),
• decreased peristalsis (decreased food
digestion)
• dilation of bronchioles
• constricts blood flow to the skin
• sweating
92
Sympathetic Division
• E.g. when running, ↑heart rate =
sympathetic.
• When hot sweat = sympathetic.
• The term “Fight or Flight” is inaccurate; it
refers to the ↑ heart rate, etc, but the
sympathetic division is also active when
relaxing on a nice beach with a cool drink on
a hot day, because whenever you’re
sweating, that’s the sympathetic division.
• Sympathetic NS and sympathy are
opposites. They should call it the ANTI93
sympathetic system.
94
ANATOMY OF THE
SYMPATHETIC DIVISION
• The sympathetic neurons exit the spinal cord at the
thorax and lumbar regions.
• The axons of most pre-ganglionic neurons in the
sympathetic division are fairly short, and they synapse
quickly on a ganglia.
• All these ganglia are lined up along the vertebral column
and are called the SYMPATHETIC TRUNK (CHAIN)
GANGLIA.
• Therefore, the postganglionic cell bodies of the
sympathetic nervous system are in the chain
ganglia.
• There are also nerves that connect the ganglia to each
other.
95
Sympathetic Trunk Ganglia
96
Sympathetic Division
In Sympathetic division,
preganglionic axons are
SHORT because they
terminate in ganglia that
are close to the spinal
cord
That means the postganglionic axons are
LONG, because they have
to reach all the way to the
97
target muscle.
Sympathetic Division
• The axons of POST-GANGLIONIC NERVES are
very long, and go to the target organs.
• Some pre-ganglionic neurons go into to the
abdomen.
• They create a group of ganglia in the abdomen
called the SOLAR PLEXUS (“sun”).
• When you get punched in the abdomen, you are
punched in the solar plexus, and get the wind
knocked out of you. It causes the diaphragm to
go into spasm.
98
PARASYMPATHETIC DIVISION
• Unlike the sympathetic division, the axons of the
preganglionic neurons of the parasympathetic
division are long, and the axons of the
postganglionic neurons are short.
• The nerve cell bodies (peripheral ganglia) of
the parasympathetic division are closer to
the organs being innervated than in the
sympathetic division.
• In fact, the cell bodies are either next to or
inside of the target organs. Therefore, they
have short post-ganglionic fibers.
99
Parasympathetic Division
In the Parasympathetic
division, preganglionic
axons are LONG
because they terminate
in ganglia that are close
to the target organ
That means the postganglionic axons are
SHORT
100
PARASYMPATHETIC DIVISION
• “Rest and Digest”
• Involved in vegetative activities, such as
digestion, voluntary urination and defecation
• Has postganglionic cell bodies in terminal
ganglia, located either near or within target
organs
• Has both preganglionic and postganglionic
neurons that secrete acetylcholine
• Has preganglionic cell bodies located in the
cervical (Vagus nerve) and sacral areas.
101
Parasympathetic Division
• The function of this division is often antagonistic
(opposite) of the sympathetic, but actually, they
work together.
• The parasympathetic division inhibits cardiac
contraction, so there is: ↓heart rate, constricts
bronchioles, activates digestive system, and
causes salivation, urination, and defecation.
• When you are lounging on the beach, the heart
rate decreases (parasympathetic), but the sweat
increases (sympathetic).
102
Vagus Nerve
• The parasympathetic neurons come out of
either the brain or the sacral region of the
spinal cord.
• The majority of the parasympathetic
outflow from the head is by the vagus
nerve.
103
Vasovagal Syncope (Fainting)
• The most common type of fainting.
• After a stressful trigger, the parasympathetic nervous
system is enhanced by the Vagus nerve.
• The heart rate speeds up, then suddenly drops.
• Then the blood pressure drops.
• Unconsciousness results.
• Treatment: elevate the legs above the heart for a few
minutes, and make sure the airway remains open.
• A cold, wet cloth on the forehead and back of the neck
may make the person feel better as they recover.
104
Path of the Vagus Nerve
105
Reynaud's Phenomenon
• Autonomic nervous system
(sympathetic division) is
hyperactive in the ANS
neurons that innervate the
walls of blood vessels.
• It causes spasms of peripheral
blood vessels, cuts off some
blood supply, and causes the
fingers and toes to be white or
blue.
• Emotional stress and being
cold tend to trigger the
discoloration.
106
Other things that can cause
vasoconstriction: Caffeine
• With frequent use, tolerance to many of the
effects of caffeine will develop. Caffeine
causes vasoconstriction. In doses of 600
milligrams (about six cups of coffee) or more
daily, caffeine can cause nervousness,
sweating, tenseness, upset stomach,
anxiety, and insomnia. It can also prevent
clear thinking and increase the side effects of
certain medications. This level of caffeine
intake represents a significant health risk. 107
Caffeine
• Caffeine can be mildly addictive. Even
when moderate amounts of caffeine are
withdrawn for 18 to 24 hours, one may feel
symptoms such as headache, fatigue,
irritability, depression, and poor
concentration. The symptoms peak within
24 to 48 hours and progressively decrease
over the course of a week. To minimize
withdrawal symptoms, experts recommend
reducing caffeine intake gradually.
108
Caffeine
• At levels over 200 milligrams per day, caffeine may delay
conception and doubles the risk of miscarriages and low
birth weight babies.
• Black tea and green tea are also dangerous, despite what you
see on the market today. Herbal tea is ok. Caffeine and tannin
in tea decreases iron and protein absorption, and is especially
dangerous during pregnancy. Black tea during pregnancy
causes birth defects.
• Caffeine taken during pregnancy is thought to increase the
probability of a child contracting diabetes.
• Because children have developing nervous systems, it is
important to moderate their caffeine consumption.
109
110
Caffeine, per cup
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Ammo: 1140 mg
Redline Power Rush: 946 mg
Expresso: 500 mg
Jolt Energy: 300 mg
Rockstar Energy: 160 mg
Coffee: 100 mg
Red Bull: 80 mg
Mountain Dew: 60 mg
Green tea: 50 mg
Tea: 50 mg
Coke: 37 mg
Dark Chocolate (1.5 oz): 20 mg
Milk Chocolate (1.5 oz): 9 mg
Hot Chocolate: 5 mg
Root Beer, Ginger ale, Lemon-Lime: 0 mg
The Ammo and Redline
manufacturers recommend
users dilute the concentrated
energy drink prior to
consumption. They also
claim that drinkers should
not just drink the shot
straight out of the bottle due
to the extreme potency!
Symptoms of Excess Caffeine
• nervousness
• anxiety
• irritability
• agitation
• tremors
• insomnia
• depression
headache
upset stomach
GI irritation
heartburn
diarrhea
fatigue
dizziness
increased heart rate
irregular heartbeat
elevated BP
increased cholesterol
nutritional deficiencies
poor concentration
bed wetting
111
Caffeine Withdrawal Symptoms
•
•
•
•
•
•
•
headache
craving
irritability
insomnia
fatigue
depression
apathy
constipation
runny nose
anxiety
nausea
nervousness
vomiting
shakiness
cramps
dizziness
ears ringing
drowsiness
hot and cold
inability to concentrate
112