Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
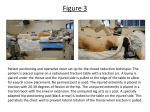
Traction Spine Pain with Radiculopathy • Neurological deficits – Mechanical compromise – Ischaemia of the nerve nerve root/nerve/dorsal root • Mechanical compromise of venous outflow • Ischemia and fibrosis – Inflammation of the nerve root/nerve/dorsal root • Intervertebral disc lesion/disease • Osteophytic encroachment • Facet inflammation – Chemical response of the nerve to nucleus material Hypothesis of Traction Biomechanical • Intervertebral Separation • Reduction of disc protrusion • Altered Intradiscal pressure • Normalization of conduction • Increased Joint Mobility Neurophysiological • Pain Relief • Decrease of Radicular symptoms Intervertebral Separation • Strong in vivo and in vitro evidence of separation of intervertebral segments • 9kg (20lbs)for 30 minutes to l-spine in vitro • Most with hips 90º/ cervical ~30º • In vivo occurred at 50lbs • Clinical Implications are unknown » Colachis & Strohm 1969, Twomey 1985, Lee & Evans 1993 Reduction of Disc Protrusion • Weak Evidence • Contrast dye injected in 3 patients • Pre and post traction radiographs • Saw reduction gone in 14 minutes • • • • Study re-done in 1992 with CT 4 patients with traction until recovery 2 had disc reduction/ 2 did not All recovered Altered Intradiscal Pressure • Weak Evidence – Single study of healthy discs – No pressure change with mechanical – Increased pressure with patient generated traction (500N) • Anderson et al 1983 Normalization of Conduction • Weak Evidence and Mixed Results – Some authors show normalized sensation, reflexes and muscle power others do not – Increased intervertebral foramen • Reducing ischemia to nerve • Improving removal of inflammatory agents • Reduce mechanical compression • Knutsson 1988, Onel 1989, Tesio 1989, Pal 1986 Increased Joint Mobility • Transitory Increase in cervical range following traction • Elongation of tissue is greater in healthy than in presence of DJD • Longer duration needed (30min) in old vs young » Some evidence for transitory increases Neurophysiological • Ectopic Impulse Generators – Spontaneous signals in dorsal root resulting from inflammation – Separation may silence these impusles – Mechanical stimulation of large diameter fibers overrides DRG • Moderate evidence in the animal model » Howe 1977, Bini 1984 Neurophysiological • Response to Pain Generation – Central Sensitization – Expansion of Receptive Fields • Thamus and PAG (decreased inhibition) – Peripheral Receptor Hyperactivity • Hypothesis of Traction effects – Increased non-nociceptive input – Recruitment of descending inhibition » Untested Application of Traction • Patient Selection • Radiculopathy – Nerve root – Stenosis – Worsens with active movement testing • Acute Phase (<6 – 12 wks) • Don’t rule out long standing (stenosis) When to Traction in Radiculopathy When to Traction in Radiculopathy When to Traction in Referred pain Headache and Traction Traction Dose • Type of Traction – Mechanical vs. Manual – At 25lbs cervical traction for radicular and non radicular complaints • No difference between intermittent, static and manual Traction Dose • Magnitude – Minimum needed to achieve goal • ~20-50% BW needed to separate IV • ~4% BW needed to overcome friction – Split table reduces friction – Split table at level of most desired traction • Cervical- 20-25lbs to overcome lordosis – 50lbs had greater separation than 30 Traction Dose • Duration – Minimum needed to achieve goal • Static vs Intermittent – Some evidence need static to overcome muscle contraction – Intermittent often less aggressive and less rebound at end Traction Dose • Body Position – Best for goal • Angle of the pull – Level – Up at an angle Flexion Worsens • Prone Traction Extension Worsens • Supine Traction Monitoring Response • • • • • • Oswestry Neck Disability Index MMT Reflexes Centralization Pain complaints • Immediate vs over 2-3 Tx’s Contraindications • Compromised spinal integrity – Malignancy, osteporosis, tumor, infection • • • • Unstable fracture Ligamentous instability (ie alar lig) Recent Fusion (3-6mo) Pregnancy (when can’t use belts) Precautions • • • • Loose fitting dentures (remove) Respiratory conditions Claustophobia Early pregnancy – May consider manual traction Traction Options • Occipital head contact • Chin halter strap • Autotraction – Pelvis is secure and traction forces are generated by grasping and pulling and pushing on bars on the ends of the table Traction Options • Positional Traction – Self unweighting on desk or counter Case • 60 year old with back and leg pain – Left buttock, anterior knee and big toe • Symptoms provoked – Walking < 1 mile – Standing 10-15 minutes • Symptoms increase – Squatting – Sitting Case 60 year old • Oswestry 16% • • • • LQS Left Quad and HS 4+/5 compared to R All other = B and Reflexes =B Sensation- Slight decrease L3 and S1 on Left Movement Testing • Asymmetrical sidebending (decreased L) – Recreates buttock pain • Flexion and Extension 75% limited pain-free – Left deviation with forward flexion • Repeated L sidebending increases tingling in toe – symptoms resolve on standing • L Quadrant closing recreates foot symptoms – Symptoms resolve when return to standing Joint Play • L2 and L3 Hypomobile • L4, L5 N • L5/S1 Unilateral – Recreates buttock pain • L4/5 Unilateral – Sore with empty end feel Special Tests • SLR (-) • Slump Test (+) Left – Recreates Buttock Pain • Palpation to piriformis – Recreates buttock c/o Case • What do you suspect is wrong? • What category does he fall into? • What will his treatment program look like? Case • Asymmetrical Sidebending • Status Quo or Worsen • Indication of Radiculopathy – May argue worsen with extension • Closing Restriction Case Treatment • Joint Mobs to Hypomoblie segments – Specific mobilizations • Traction – Mechanical effects of intervetebral separation – Parameters to maximize Treatment and Traction – 130 lbs first day- progressing to 190 over 4 treatments – 12th treatment walk greater than 1 mile with no symptoms and raquetball with no symptoms – 16th treatment- could stand to lecture today – 23rd treatment- walked around campus 3x today • Walking is fun – 25th treatment- great weekend but has buttock pain- + SIJ testing