Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
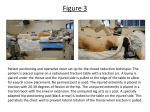
Mechanical Traction Therapeutic Modalities in Physical Therapy General Information •Traction means to draw or pull • Distraction means to separate joint surfaces Effects – Separation of vertebral bodies – Distract and glide facet joints – Tensing of the ligamentous structures – Widening of the intervertebral foramen – Straightening of spinal curves – Stretching of spinal musculature Types of Traction • Continuous – Tx applied for several hours at a time – Constant tension – Limited weight tolerated due to long duration – Ineffective in creating separation – Normally applied with suspended weights Types of Traction • Sustained (static) – Tx applied with constant tension for several minutes up to ½ hour – May be applied via suspended weights or a mechanical device Types of Traction • Intermittent Mechanical – Tx applied via a mechanical device with tension alternately applied and then released – Termed hold and rest – Hold and rest times usually vary from a few seconds up to 1 minute Types of Traction • Manual – Tx applied by the therapist grasping the patient and utilizing his or her own force to create traction – May be applied for a several second hold or as a quick thrust – Limited by strength and endurance of the therapist – Very accommodating and provides feedback – Some possible apprehension by patient Types of Traction • Positional – Tx applied by use of gravity and positioning to effect spinal structures with minimal intervention – Utilizes pillows, blocks, bolsters – Normally has a unilateral effect Types of Traction • Gravity – Tx utilizing the force of gravity acting on the patients body weight to effect spinal structures – 2 types: • Vest that suspends the lower body by exerting pressure on the rib cage • Boots that attach to a rod at the ankles with patient in inverted position Treatment Indications • Disc herniation – In an erect posture the disc helps to dissipate compressive forces – With movement into flexion/extension/lateral flexion, the pressure changes Treatment Indications • Nucleus pulposus does not move – With rupture of the annulus fibrosis the nucleus is allowed to move out of the intervertebral space – Increases space available, creates suction force, and allows fluid exchange to get rid of waste and allow in fresh nutrients – Effects are transient Treatment Indications • Reversed with weight bearing and flexion (corset, brace) – Need neutral spine position to get disc back in – Extension maintained for scar tissue formation – Some researchers report increased fluid in the nucleus pulposus drawn from the vertebral body during tx – This will explain the increase in pain in some patients with disc prolapses, immediately following tx – They recommend using 30 pounds as an initial tx force with disc patients to assess their tolerance Treatment Indications • Degenerative disc disease – Narrowing of intervertebral spaces – Pressure on nerve roots, increased load on facets – Traction widens space and decreases pressure temporarily – May result in realignment that decreases pressure Treatment Indications • impinged capsule • Joint hypomobility – Mobilization, passive joint movement, nonspecific – Pain control by synovial fluid exchange to facet capsules and the meniscus for nutrition, and proprioceptive response from moving facet structures gives a gate control response Treatment Indications • Nerve root impingement – From bulging disc, osteophytes (spurs), narrowed foramen – Tingling usually associated with nerve compression – Continued pressure gives demyelination with slowing of nerve impulses and can progress to axon death with resulting numbness, weakness and diminished reflex responses – Muscle spasms may develop in paraspinals with the same innervation level – Widens foramen – May need unilateral or rotation added – May realign to decrease pressure – Decreases spasms that may be the cause of compression – Nerve irritation can cause muscle spasms as the root levels may be the same, just different axons Treatment Indications • Muscle tightness, spasms – Stretches, inhibits – Decreases load on other structures (nerve root, facets, disc) that may result in spasms – Fluid exchange – Initial stretch should come form positioning – EMG activity will decrease with proper technique, increase with improper Treatment Indications • Scoliosis – Pulls towards a more correct alignment – Stretches out tight musculature or other joint structures • Pain – Traction may decrease pressure on sensitive structures and give a gate control effect with movement of these structures Contraindications • Acute conditions – Tx to acute sprains and strains may overwhelm already weakened soft tissue • Already weakened soft tissue • Joint instability – hypermobility • Structural disease secondary to infection, tumor, etc. • Vascular compromise • Fractures • Tumors • Bone disease or infection • Cardiac conditions Relative Contraindications • Pregnancy • Osteoporosis • Hiatal hernia • Claustrophobia General Technique for Applying Lumbar Tx • Force must be great enough to effect change to the target structure – 20-50% to move body – Coefficient of friction is about 0.5 – Usually attempt to move 50% of the patient’s body weight – 65-100 lbs of force to separate vertebrae on average • May not be necessary for all treatments (spasms, pain) • May not get to 65-100 lbs on first treatment – Split table to reduce friction, must separate at target tissue – Damage not reported until somewhere in the 400-800 lb range – Instability is a problem with the sedentary, weak, elderly, and young General Technique for Applying Lumbar Tx • Patient must be able to relax – Cannot out pull musculature – No pain – Use adjunctive treatments – Research shows a decrease in joint space with poor traction technique – EMG activity will increase with a pull that is too strong or with poor, uncomfortable positioning General Technique for Applying Lumbar Tx • Traction harness use – Clip buckle versus velcro – Vinyl versus cotton – Adjustable lengths, pads – Placement of lumbar belts • skin versus clothes – dissipate traction force) – Use of thoracic belts on lower, lateral ribs • Not in axilla – The thoracic belt is placed on after the pelvic belt General Technique for Applying Lumbar Tx • Patient position – Prone versus supine (comfort, goals) – Prone • Disc • Pillows under abdomen to flatten lordosis, under thighs or chest to increase extension – Supine • Mobilization • pillows under knees to decrease lordosis – Initial soft tissue stretch on soft tissue should come from positioning General Technique for Applying Lumbar Tx • Adjustments to belts, positioning and poundage – Made with first few pulls before split table is released – All slack is taken up before table is released and release is only during rest phase Effects of Lordosis (supine) • Leg Position – Up on a stool, decreases lordosis – Flat, normal lordosis is maintained – 90/90 position should flatten back, less than that decreases in increments • Rope Angle – Flat low pull maintains – With increased (elevated) rope angle, lordosis decreases • Pelvic Harness – Greatest effect on lordosis – Posterior pull decreases lordosis – Lateral pull maintains lordosis – Anterior pull increases lordosis – Positions between these will result in incremental changes Effects on Lordosis (prone) • Patients with sever pain and muscle spasms may tolerate prone traction better • Pillows and harness to control lordosis • Rope angle – Always low – Pillows can decrease or increase lordosis • Pelvic harness – May be placed to effect lordosis, as with supine – Harness is never placed posteriorly in prone – Rarely anterior – As a rule, it is placed laterally to maintain other positional effects • Treatment in prone – Allows performance of other modalities without position changes – Allows for easy palpation of the interspinous spaces to determine the level and degree of spinal motion Traction Type (mode) • Sustained – Well suited for disc herniations, muscle spasms other soft tissue tightness – Less poundage is tolerated than with intermittent – Mechanical devices are most effective – Pulleys with weights do not take up slack well over time to sustain constant tension Traction Type (mode) • New digital tx devices – Are programmable – Poundage (tension) can be increased in steps pre-set by therapist – Protocols for hold/rest times, steps to increase tension incrementally, etc – Can all be programmed into many devices and saved – Gradual build up allows patient to accommodate to increases in tension – Studies show a greater degree of ligament deformation with a low rate of loading compared to a more rapid rate – Long term shortening with contractures from positioning over the years responds well to this low rate Traction Type (mode) • Intermittent – Patients can tolerate greater poundages with the rest periods – Works well for joint hypomobility and degenerative disc disease with shorter rest and hold times (mobilizing effect) Traction Type (mode) • Positional – Normally sidelying over a bolster or blanket – Well suited for scoliosis treatment and other long term treatments – Can be performed at home by the patient – If tightness is severe enough, the tightened structures may result in a scoliosis – Concavity will be on the tight side – Patient is placed in sidelying on the convex side with the apex of the curve on the bolster – Allows gravity to effect a traction force on the patient’s body weight – Creates unilateral separation on the opposite side of the spine – Flexion of the hips and knees to forward bend the spine – Trunk rotation towards the side of the superior shoulder will increase the opening of the spine on that side – In supine, with hips and knees flexed allows opening of the intervertebral foramen, bilaterally – Also useful with patients on very restricted activity due to pain Traction Type (mode) • Manual – Very adaptable – Various angles may be applied with combinations of rotation, long axis distraction, lateral flexion and flexion/extension – Allows tx to be applied to a specific level as it is palpated – May be utilized as a evaluation tool to aid in determining a diagnosis and to assess tolerance and effectiveness of traction – Limited by strength and endurance of therapist – Better suited for cervical than lumbar traction – Allows constant adjustments by the therapist based on constant feedback – Can be applied unilaterally to one leg to effect the iliofemoral joint or the sacroiliac joint Treatment Time • Generally 20 minutes for sustained or intermittent • May be adjusted downward as tolerated, especially with initial treatments • Disc: 8 minutes or less if sustained tx is used • Traction creates a suction force as vertebrae are separated, pulls disc back in place – suction effect is eliminated with time as pressures across membrane equalize Cervical Traction • Objectives and concepts are much the same as for lumbar traction • Some adjustments are required in techniques of application and occurrence rates of particular dysfunctions vary (less disc, more ligamentous) • In the cervical spine, the vertebral arteries, part of the blood supply to the brain, lie within the bony structures of the spine Positioning for Cervical Tx • Sitting – Less desirable, but occasionally necessary • Ex. Necessary with reflux esophagitis – Unable to relax musculature – Halter pulls on mandible, puts pressure on TMJ – Flexion is applied by use of a posterior tilting traction chair or by the use of pillows behind the low back, sliding the hips forward and resulting in forward flexion of the neck when the traction force is vertical Positioning for Cervical Tx • Supine – In halter, more load is placed on the occiput by gravity – Increased ability to relax – Facilitates the use of Saunders and other new devices which avoid TMJ loading – Position of choice – 20-30 degrees of flexion is needed to place the spine in neutral and flatten the normal lordosis – Exception is treatment to the atlanto-axial and atlantooccipital joints • These joints should be treated with maintenance of the normal lordosis of the cervical spine according to Saunders Effects on Cervical Flexion • Rope Angle – To effect 25-30 degrees of flexion on the neck the rope angle will need to approach 45 degrees due to the flexibility of the rope resulting in a sagging with the weight of the head – The angle is 0, or flat for atlanto-occipital and atlanto-axial traction General Technique for Applying Cervical Tx • Halter – The position of the halter will have the most significant effect on cervical spine flexion – A halter placed and tightened too low on the neck will result in head on neck extension and the inability to eliminate the cervical lordosis – A halter placed to high on or past the occiput or placed too loosely will slip off when a traction force is applied – Ideally, the occipital pad is placed directly on the occiput and tightened snugly enough to prevent slipping – A poor set-up will result in head on neck extension and uncomfortable loading of the mandible and in effect the TMJ – Halters should not be utilized on patients with a history of TMJ dysfunction or patients with poor dental occlusion General Technique for Applying Cervical Tx • Saunders – Saunders or similar traction devices utilize a sliding track, with placement of the head on a pad on the carriage to decrease the tension load necessary to produce a traction force by eliminating most of the friction – Stabilization is provided by a head strap and posterior pads that are tightened against the occiput and the mastoid processes General Technique for Applying Cervical Tx Poundage – Research reports separation of vertebral bodies with ranges from 25-40 pounds – 10 pounds for the atlanto-occipital and atlanto-axial joints – Cadaveric studies did not show damage until 120 pounds of traction – Less than 25 pounds may be effective if separation of vertebral bodies is not the goal – Stretching of posterior musculature and opening of the intervertebral foramen can occur at lesser poundages – Normally greater than 10 pounds is required just to offset the weight of the head General Technique for Applying Cervical Tx Manual Traction • Can be highly effective in the cervical spine with good orthopaedic skills • Highly flexible, constant feedback • High load on the therapist • Manual traction also allows for pressure over trigger points for pain control as traction is being applied