Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
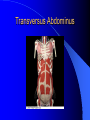
Establishing Core Stability in Rehabilitation Chapter 5 Objectives Definitions Origins Benefits Theory/Posture and anatomy Research Practical WHAT IS CORE STABILITY? “The system the body uses to give spinal support and maintain muscular balance while at the same time providing a firm base of support from which other muscles can work to enable the body to undertake its daily tasks. It is through this system of joint integrity and support that the body is able to maintain its posture – the position from which all movement begins and ends” Chek P. 2000 What is the CORE? Lumbo-pelvic-hip complex Location of center of gravity (CoG) Efficient core allows for Maintenance of normal length-tension relationships Maintenance of normal force couples Maintenance of optimal arthrokinematics Optimal efficiency in entire kinetic chain during movement Acceleration, deceleration, dynamic stabilization Proximal stability for movement of extremities CORE STABILITY “The ability to maintain neutral spine using the abdominal, back, neck and shoulder girdle muscles as stabilisers rather than movers” Orthopaedic view “That state of muscular and skeletal balance which protects the supporting structures of the body against injury or progressive deformity, irrespective of the attitude in which these structures are working or resting” Academy of Orthopaedic Surgeons 1947. NOT A NEW CONCEPT STATIC • Alexander Technique Pilates DYNAMIC Tai-chi/Karate Swiss ball training ALEXANDER TECHNIQUE 1869-1955 PRINCIPLES – RE-EDUCATION OF KINAESTHETIC SENSE – QUIETING THE MIND TO FOCUS ON THE MIND/BODY CONNECTION – ESTABLISHING A GOOD HEAD AND NECK POSITION JOSEPH PILATES 1880-1967 PRINCIPLES – – – – – CONCENTRATION ALIGNMENT BREATHING CO-ORDINATION STAMINA FITNESS PARAMETERS CARDIOVASCULAR STRENGTH / POWER/SPEED ENDURANCE FLEXIBILITY CORE STABILITY PROPRIOCEPTION / NEUROMUSCULAR CONTROL Paradigm Shift: No longer looking to improve strength in one muscle but improvement in multidirectional multidimensional neuromuscular efficiency (firing patterns in entire kinetic chain within complex motor patterns). The Theories Spinal Stability The passively supported spine (bone and ligament will collapse under 20lb (9kg) of load. Muscular components that contribute to lumbo-pelvic stability which take up the slack Control subsystem (Neural) Spinal stability Passive subsystem (spinal column) Active subsystem (spinal muscles) Adapted from Panjabi (1992) Neutral Zone Concept Every joint has a neutral zone or position Overall internal stresses and muscular efforts are minimal A region of intervertebral motion around the neutral position where little resistance is offered by the passive spinal column (Panjabi 1992) •Movement outside this region is limited by the ligamentous structures providing restraint Control of the Neutral Zone Ligaments - support end of range only - Can be unstable/over-stretched Muscle - Can compensate for instability Increase the stiffness of the spine Decrease the neutral zone Form basis for therapeutic intervention in treatment of spinal stability Clinical instability • A significant decrease in the capacity of the stabilising system of the spine to maintain the internal neutral zones within physiological limits which results in pain and disability (Panjabi) Patho-Kinesiological model Muscular system Articular system Neural system All three must work as an integrated unit The movement system requires optimum function of the core stabilisers resulting in precise arthokinematics and osteokinematics (Sarhmann 2000) Spinal Stability Demonstrated that submaximal levels of muscle activation adequate to provide effective spinal stabilisation Continuous submaximal muscle activation crucial in maintaining lumbopelvic stability for most daily tasks. Benefits of Spinal Stability Improve Posture and prevent deformities More stable Centre of Gravity and control during dynamic movements contribute to optimal movement patterns breathing efficiency Distribution of forces and absorption of forces Reduce stress on joint surfaces and pain Injury prevention and rehabilitation Improved Posture Re-education of stabilisers Reduced stress on joints Reduced injury Increase function and sports performance. For Sporting Performance •Forces transmitted - trunk to the limbs •Core muscles support the spine to transmit power from the trunk. •Power is transferred for kicking and throwing activities •If the peripheral limbs are too heavy this will cause stress on the chassis 29 muscles attach to core Lumbar Spine Muscles Transversospinalis group Rotatores Interspinales Intertransversarii Semispinalis Multifidus Erector spinae Iliocostalis Longissimus Spinalis Quadratus lumborum Latissimus Dorsi Functional Anatomy Transversospinalis group Poor mechanical advantage relative to movement production Primarily Type I muscle fibers with high degree of muscle spindles Optimal for providing proprioceptive information to CNS Inter/intra-segmental stabilization Erector spinae Provide intersegmental stabilization Eccentrically decelerate trunk flexion & rotation Quadratus Lumborum Frontal plane stabilizer Works in conjunction with gluteus medius & tensor fascia latae Latissimus Dorsi Bridge between upper extremity & core Abdominal Muscles Rectus abdominus External obliques Internal obliques Transverse abdominus Work to optimize spinal mechanics Provide sagittal, frontal & transverse plane stabilization STABILISING CORE MUSCLES THE INNER CORE Transversus abdominus Multifidus Pelvic Floor Muscles Diaphragm The Outer Core Systems Anterior Oblique – ext and int obliques and contralateral hip adductors connected by anterior abdominal fascia Posterior Oblique – Lat Dorsi and contralateral Glut Max connected by T/L fascia Deep Longitudinal – Erector spinae and c/l sacrotubrous ligament and biceps femoris (connected by T/L fascia) Lateral – Glut med and min and c/l adductors TRANSVERSUS ABDOMINUS Transversus Abdominus