Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
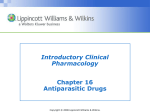
Management of Patients With Infectious Diseases 1 Copyright © 2008 Lippincott Williams & Wilkins. Chain of Infection 2 Copyright © 2008 Lippincott Williams & Wilkins. Causes of Infection • Bacteria (eg, streptococci) • Viruses (eg, hepatitis B) – Not cells – Contain RNA or DNA, can only reproduce inside a living cell • Fungi (eg, Candida) – Organisms similar to plants • Protozoa (eg, Giardia) – Single celled, animal-like organisms 3 Copyright © 2008 Lippincott Williams & Wilkins. Colonization, Infection, and Disease • Colonization: describes microorganisms present without host inference or interaction (eg, S. aureus lives on skin - “colonized”) • Infection: indicates host interaction with the organism (eg, bacteria enters wound, causes local inflammation) • Disease: the infected host displays a decline in wellness due to the infection (eg, 10 of people infected with TB have clinically significant disease) 4 Copyright © 2008 Lippincott Williams & Wilkins. Biologic spectrum of Response to Bacterial Infection at the Cellular Level and of the Intact Host 5 Copyright © 2008 Lippincott Williams & Wilkins. Interpreting the Microbiology Report • A tool to determine colonization, infection, or disease • The organism reported may reflect colonization rather than infection • Mix of cells in smear and stain report may indicate cellular response • Culture and sensitivity specify the organism and which antibiotic will inhibit growth • Analyze results in conjunction with the clinical 6 assessment of the patient Copyright © 2008 Lippincott Williams & Wilkins. Information Resources • World Health Organization (WHO) • Center for Disease Control and Prevention (CDC) – CDC publications, guidelines, and internet site • Occupational Safety and Health Administration (OSHA) – Mandatory regulations and guidelines for the workplace • Local agencies, such as county facilities • Hospital/facility infection control specialists and facility policies 7 Copyright © 2008 Lippincott Williams & Wilkins. Infection Precautions • Guidelines to prevent the transmission of microorganisms in hospitals • Standard precautions used for all patients – The primary strategy for preventing hospital-acquired infections (nosocomial infections) – Applies to blood, all body fluids, nonintact skin, and mucous membranes • Transmission-based precautions are for patients with known or suspected infectious diseases spread by 8 airborne, droplet, or contact routes Copyright © 2008 Lippincott Williams & Wilkins. Elements of Infection Precautions (see table 15-9) • Hand hygiene • Use of gloves and other barriers • Mask, eye protection, face shield • Gown • Proper handling of patient care equipment and linen • Environmental control • Prevention of injury from sharps and needles Copyright © 2008 Lippincott Williams & Wilkins. 9 Transmission-Based Precautions • Airborne precautions – Hospitalized patient should be in negative pressure room with the door closed; health care providers may need to wear an N-95 respirator (mask) when in the room (eg, Varicella and TB) • Droplet precautions – Wear a face mask but door may remain open; transmission is limited to close contact (eg, pertussis, influenza) • Contact precautions – Use of barriers to prevent transmission; emphasize cautious technique as organism is easily transmitted by contact between the health care worker and the patient 10 (eg, C. diff, VRE, impetigo) Copyright © 2008 Lippincott Williams & Wilkins. Specific organisms with HealthCare Associated Potential • Clostridium difficile – Usually results as a superinfection in patients on antibiotic therapy; kills off “good bacteria” in the gut and result in overgrowth and infection with C. difficile – Manifests as diarrhea, possible colitis and sepsis • Methicillin-resistant Staphylococcus aureus (MRSA) • Vancomycin-resistant Enterococcus (VRE) – MRSA and VRE are drug-resistant bacteria common in healthcare facilities; also emerging in community settings – Often transmitted to patients via healthcare workers • See table 15-7 for patient teaching Copyright © 2008 Lippincott Williams & Wilkins. 11 Health-Care Associated (Nosocomial) Bloodstream Infections • High morbidity and mortality • Most often due to vascular access device – Bacteremia – Fungemia (less common, poor prognosis) • Prevention – – – – – Hand hygiene Strict sterile technique during insertion Strict sterile technique during dressing change Skin disinfection Infusion set and stopcocks changed per hospital policy 12 Copyright © 2008 Lippincott Williams & Wilkins. Emerging Infections • A disease whose incidence has increased in the past 20 years or threatens to increase in the immediate future – – – – – – Severe Acute Respiratory Syndrome (SARS) West Nile Virus Lyme disease HIV Hepatitis C H1N1 influenza 13 Copyright © 2008 Lippincott Williams & Wilkins. Reemerging Infections • Vaccines and proper medications have led to near eradication of some infections, which have the potential to reemerge under the right condition – Tuberculosis – Pertussis (whooping cough) – Dengue fevver – Giardiasis 14 Copyright © 2008 Lippincott Williams & Wilkins. Vaccinations (see handouts) • Goal is to use wide-scale efforts to prevent specific infectious diseases from occurring in the population • Common vaccines – – – – – – – Measles, mumps, rubella Varicella Influenza Tetanus, diptheria Pneumococcal Meningococcal Hepatitis B 15 Copyright © 2008 Lippincott Williams & Wilkins. Vaccinations • Contraindications of vaccines – Anaphylaxis from previous dose – Live vaccines are contraindicated for patients with severe immunosuppression (eg, HIV, leukemia, immunosuppresant medications) – MMR contraindicated in pregnant women 16 Copyright © 2008 Lippincott Williams & Wilkins. Sexually Transmitted Diseases • Acquired through sexual contact with an infected person – Portals include skin and mucosal linings of the urethra, cervix, vagina, rectum and oropharynx • 19 million Americans become infected annually • Risk reduction – Use of latex condoms – Minimize number of sexual partners – Screening high risk individuals 17 Copyright © 2008 Lippincott Williams & Wilkins. Sexually Transmitted Diseases • Syphilis ( caused by Treponema pallidum, a spirochete) – Primary syphilis (3-8 weeks) • Chancre at site of entry – Secondary syphilis (1-2 years) • Rash, flu-like symptoms, condylomata lata, adenopathy – Latency period (3 - 20 years; may be permanent) • Absent signs and symptoms 18 Copyright © 2008 Lippincott Williams & Wilkins. Sexually Transmitted Diseases – Tertiary syphilis (chronic, may be fatal) • Gumma, cardiac (aortic aneurysms, aortitis), neurosyhpillis (psychosis, stroke, paresis) • Diagnosis • RPR or VDRL; other treponemal tests – Treatment • Penicillin G; doxycycline if allergic 19 Copyright © 2008 Lippincott Williams & Wilkins. Primary Syphillis - Chancre 20 Copyright © 2008 Lippincott Williams & Wilkins. Sexually Transmitted Diseases • Chlamydia trachomatis and Neisseria gonorrhoeae – Common bacterial STDs • Clinical manifestations – Women often asymptomatic; may have purulent discharge, or symptoms of UTI – Men may also be asymptomatic; may have burning with urination and penile discharge, painful testicles, epididymitis • Complications – Women - pelvic inflammatory disease (PID), endometriosis, infertility – Men-epididymitis 21 – Both - arthritis Copyright © 2008 Lippincott Williams & Wilkins. Sexually Transmitted Diseases • Chlamydia trachomatis and Neisseria gonorrhoeae • Diagnosis – Gram stain and culture of genital secretions; anal or oropharynx secretions if indicated – CDC recommends routine screening of all pregnant women and women < 26 years • Treatment – – – – Due to frequent coinfection, treatment should cover both! Chlamydia: azithromycin or doxycycline preferred Gonorrhea: ceftriaxone, cefixime ciprofloxacin, ofloxacin All sexual partners must be treated 22 Copyright © 2008 Lippincott Williams & Wilkins. Sexually Transmitted Diseases • Herpes simplex virus – Type I (“on the face”) • May cause cold sores – Type II (“below the waist”) • May cause genital ulceration • Many asymptomatic – *Either virus can cause disease on the mouth or genitals* – Lifelong carrier; primary episode and recurrent episodes • Treatment may reduce viral activity – Acyclovir, valcyclovir, famciclovir – Barrier protection to prevent transmission 23 Copyright © 2008 Lippincott Williams & Wilkins. Genital Herpes 24 Copyright © 2008 Lippincott Williams & Wilkins. Nursing Process—Assessment of the Patient With Sexually Transmitted Disease (STD) • Protecting confidentiality and privacy is an important component in the assessment of a patient with STDs • Communication needs to be culturally and emotionally sensitive and clarification of terms may be necessary • Presenting symptoms • Specific information regarding sexual contacts • Patient knowledge • Physical examination: include rashes, lesions, drainage, inguinal nodes, genitalia, rectum, mouth and throat; women need abdominal and uterine exams 25 Copyright © 2008 Lippincott Williams & Wilkins. Nursing Process—Diagnosis of the Patient With Sexually Transmitted Disease (STD) • Deficient knowledge • Anxiety • Noncompliance with treatment 26 Copyright © 2008 Lippincott Williams & Wilkins. Collaborative Problems/Potential Complications • Increased risk for ectopic pregnancy • Infertility • Transmission of infection • Neurosyphilis • Gonococcal meningitis • Gonococcal arthritis • HIV-related complications 27 Copyright © 2008 Lippincott Williams & Wilkins. Nursing Process—Planning the Care of the Patient With Sexually Transmitted Disease (STD) • Major goals include increased patient understanding of the natural history and treatment of the infection, reduction in anxiety, increased compliance with therapeutic and preventive goals, and absence of complications 28 Copyright © 2008 Lippincott Williams & Wilkins. Interventions • Education about STDs and the spread of infection • Reduce anxiety – Encourage patient to discuss anxieties and fears – Provide factual information and individualized teaching – Assist in planning discussion with partners – Provide referral to social worker or other specialist • Increase compliance – Provide patient teaching in group or individual settings – Provide referral to appropriate agencies Copyright © 2008 Lippincott Williams & Wilkins. 29