Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
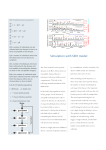
Assessing Risk from Environmental Exposure to Waterborne Pathogens: Use of Dynamic, Population-Based Analytical Methods and Models May 11, 2005 This lecture is based on lecture material prepared by Prof. Joe Eisenberg, formerly of the University of CaliforniaBerkeley and now at the University of Michigan Used with his permission Overview Role of water in disease burden – Water as a route of disease transmission Methods of risk estimation – Direct: intervention trials – Indirect: risk assessment Population-level risks – Example: the Milwaukee outbreak Importance of Waterborne Pathogens Domestic: U.S. interest in water quality – 1993 Cryptosporidium outbreak – Increasing number of disease outbreaks associated with water – Congressional mandates for water quality – (Safe Drinking Water Act) – Emphasis on risk assessment and regulation Importance of Waterborne Pathogens Worldwide: WHO interest in water quality – Estimating GBD associated with water, sanitation, and hygiene – Diarrheal diseases are a major cause of childhood death in developing countries. – 3 million of the 12.9 million deaths in children under the age of 5 attributable to diarrheal disease – Emphasis on intervention and control Pathways of Transmission Person-person – Mediated through fomites (e.g., phone, sink, etc.) – Often associated with hygiene practices Person-environment-person – Mediated through water, food, or soil – Contamination can occur through improper sanitation (example: sewage inflow into drinking water source or lack of latrines) – Animals are often sources (Zoonotic pathogens) – Exposure can occur through improper treatment of food or water The Disease Transmission Process Risk estimation depends on transmission dynamics and exposure pathways Transport to other water sources Agricultural Runoff Drinking Water Animals 2° Trans. Food Recreational Waters or Wastewater reuse Approaches to Risk Estimation Direct approach: The intervention trial – Can be used to assess risk from drinking water and recreational water exposures – Problems with sensitivity (sample size issue) – Trials are expensive. Indirect approach: Mathematical models – Must account for properties of infectious disease processes – Pathogen specific models – Uncertainty and variability may make interpretation difficult. Approaches to Risk Estimation Combining direct and indirect approaches – Models can define the issues and help design studies. – Epidemiology can confirm current model structure and provide insight into how to improve the model. Approaches for Risk Estimation: Direct estimates of waterborne infectious illnesses Surveillance: count waterborne infectious illnesses – How can a waterborne disease outbreak be distinguished from other outbreak causes (food, fomites, etc.)? – What about endemic disease? Observational – Ecologic studies (e.g., serosurvey comparing communities with and without filtration). – Time series (e.g., correlation between turbidity and hospitalization data) Approaches for Risk Estimation: Distinguishing waterborne GI disease from other GI diseases Methods for addressing the question – In a single community: a randomized, blinded, placebocontrolled trial – design provides an estimate of the effectiveness of a drinking water intervention. Basic study design: two groups “Exposed” group = normal tap water. “Treated” group = use a water treatment device to provide water as pathogen-free as technically possible Approaches for Risk Estimation: A Tap Water Intervention Trial Enroll 1000 subjects 500 receive an active home water treatment device (and carry drinking water to work, etc. when practical) 500 receive a “placebo” home water drinking device (does nothing to change the water) Follow the subjects for one year with daily logs of GI illness Alternative design: Each household changes device type after 6 months. Approaches for Risk Estimation: A Tap Water Intervention Trial Placebo group (tap water): – 90 illnesses over course of the study – “Rate” = 90 / 500 Rate in placebo group = 0.18 per person per year Treated group (active device): 60 illnesses in the treated group (active device) “Rate” = 60 / 500 Rate in treated group = 0.12 per person per year Approaches for Risk Estimation: Epidemiologic Measures Relative Risk (RR) Incidence in exposed group Incidence in unexposed group Interpretation: the risk of disease in the tap water group is 1.5 times higher than that of the treated group Approaches for Risk Estimation: Epidemiologic Measures Attributable Risk (AR) Incidence in exposed – Incidence in unexposed Incidencetapwater Incidenceactive 0.18 0.12 0.06 Interpretation: There are 6 excess cases of disease per 100 subjects receiving tap water Approaches for Risk Estimation: Epidemiologic Measures Attributable Risk Percent (AR%) Excess cases in exposed Incidence in exposed Excess Casestapwater 0.06 0.33 Incidencetapwater 0.18 Interpretation: 33% of the cases of disease in the tap water group are due to water Approaches for Risk Estimation: Epidemiologic Measures To generalize beyond the cohort, need an estimate of the community incidence. PAR: population attributable risk PAR%: population attributable risk % AR compares completely protected group with completely unprotected group. PAR incorporates intermediate exposure Approaches for Risk Estimation: Epidemiologic Measures Population attributable risk Incidence in the community–incidence in the unexposed IncidenceComm Incidenceactive 0.14 0.12 0.02 Interpretation: In the community, 2 excess cases of disease per every 100 subjects in the community Approaches for Risk Estimation: Epidemiologic Measures Population attributable risk percentage Excess cases in the community Incidence in the exposed Excess CasesComm 0.02 0.14 Incidencetapwater 0.14 Interpretation: 14% of the cases of disease in the community are due to tap water Approaches for Risk Estimation: Tap Water Intervention Trials Trials in immunocompetent populations Canada (Payment)--challenged surface water – AR = 0.35 (Study 1), 0.14-0.4 (Study 2) Australia (Fairley)--pristine surface water – No effect Walnut Creek (UCB) – pilot trial – AR = 0.24 (non-significant effect) Iowa (UCB)--challenged surface water – No effect Trials in sensitive populations HIV+ in San Francisco (UCB)--mixed sources Elderly in Sonoma (UCB)--intermediate quality surface Approaches for Risk Estimation: Tap Water Intervention Trials Davenport, Iowa study – Comparing sham vs. active groups – AR = - 365 cases/10,000/year (CI: -2555, 1825) – Interpretation: No evidence of a significantly elevated drinking water risk – Is the drinking water safe? Approaches for Risk Estimation: Risk Assessment vs. Intervention Trial Comparing estimates from a risk assessment to randomized trial results (Eienberg et al. AJE, submitted) Data collected during the intervention trial – Self-report illnesses from participants: Weekly diaries – Source water quality: Cryptosporidium, Giardia, enteric viruses – Drinking water patterns: RDD survey – Water treatment: B. subtilis, somatic coliphage Approaches for Risk Estimation: Risk Assessment Model Approaches for Risk Estimation: Risk Assessment Model Cryptosporidium Model Giardia Viruses 1. Source water Concentration (organisms per liter) (Normal Mean (SD)*) 2.68 (24.20) 0.93 (3.00) 0.40 0.40 0.48 3.84 (0.59) 3.84 (0.59) 0 3.5 (2.93) 4 (2.93) 0.094 (0.42) 0.094 (0.42) 0.094 (0.42) 4. Dose Response § : 0.004078 : 0.01982 ,: 0.26, 0.42 5. Morbidity Ratio# 0.39 0.40 0.57 Recovery rate 1.06 (2.24) 2. Treatment efficiency (logs removal) Sedimentation and filtration (Mean (SD)*) Chlorination (Mean (SD) 3. Water Consumption 1.99 (0.52) in liters (mean (SD) ‡) Approaches for Risk Estimation: Risk Assessment Results Overall risk estimate: 14 cases/10,000/yr Table 2. Summary of risk estimates (cases/10,000,yr) Cases of Illness Mean Percentile (2.5, 97.5) Cryptosporidium 2.1 (0.8, 3.5) Giardia Enteric viruses (disinfection = 4 log removal) Enteric viruses (disinfection = 4 log removal) 3.4 (0.6, 15.5) 8.4 (0.2, 18.7) 0 (0, 0.2) Approaches for Risk Estimation: Comparison/Conclusions Table 3. Comparison of risk assessment and intervention trials Risk Assessment Intervention Trials Not relevant Low Indirect Direct Pathogen inclusion Few Many Model Specification Adds uncertainty Not relevant Transmission processes Can be included* Only in a limited way Distribution System effects Can be included* Was included Examining alternative control strategies Yes No Expense Low High Time Fast Slow Sensitivity Causal evidence * Was not included in this study Microbial Risk Assessment Two classes of risk assessment models Individual-based Population-based Individual-based estimates Risk estimates assume independence among individuals within the population Chemical risk paradigm Focus is on direct risks Probability of disease for a given individual This probability can be either daily, yearly, our lifetime. Microbial Risk Assessment Chemical risk paradigm –Hazard identification, exposure assessment, dose response, risk characterization Model structure P 1 (1 ( N )) where P = probability that a single individual, exposed to N organisms, will become infected or diseased. Exposure calculation: N V1 co e kt t 10 kd d Microbial Risk Assessment Alternative framework: risk estimates at the population level allow for the inclusion of indirect risks due to secondary transmission Transport to other water sources Agricultural Runoff Drinking Water Animals 2° Trans. Food Recreational Waters or Wastewater reuse Microbial Risk Assessment Eisenberg et al. AJE 2005 Transmission pathways – Example: a Cryptosporidium outbreak in Milwaukee Wisconsin, 1993 Competing hypotheses on the cause Oocyst contamination of drinking water influent coupled with treatment failure Chemical risk paradigm may be sufficient (still need to consider secondary transmission) Amplification of oocyst concentrations in the drinking water influent due to a person-environment-person transmission process Chemical risk paradigm cannot address this potential cause of the outbreak A model of disease transmission: The SIR model Mathematical modeling of a population where individuals fall into three main categories: Susceptible (S) Infectious (I) Recovered (R) Different individuals within this population can be in one of a few key states at any given time Susceptible to disease (S) infectious/asymptomatic (I) infectious/symptomatic (I) non-infectious/asymptomatic; recovered (R) A dynamic model: individuals are moving from state to state over time The SIR model: key details There are two sets of variables: Variables describing the states people are in S=susceptible I=infectious R=non-infectious/asymptomatic Variables describing how many people are moving between these states (parameters) Example: γ=Fraction of people in state R who move to state S The SIR Model g S I W • • • • • • • • • d R ENVIRONMENT S: Susceptible I: Infectious (symptomatic+asymptomatic) R: Non-infectious W: Concentration of pathogens in the environment β: Infection rate due to exposure to pathogen δ: Fraction of people who move from state I to state R γ: Fraction of people who move from state R to state S Solid lines: Individuals moving from state to state Dashed lines: Pathogen flows between individuals in different states The SIR Model: slightly different version g a X 0+ (W) Y λ W (ρ) ρ Z μ σ D δ+μ The variables • X: susceptible • Y: infectious/asymptomatic • Z: non-infectious/asymptomatic • D: infectious/symptomatic • W: concentration of pathogens at the source • a: number of new susceptible individuals migrating in The SIR Model: slightly different version (cont) g a X 0+ (W) Y λ W (ρ) ρ Z μ σ D δ+μ The parameters • ρ: fraction in state Y who move to state D • α: Fraction in state Y who move to state Z • σ: Fraction in state D who move to state Z • γ: Fraction in state Z who move to state X • δ: Fraction in state D who die • μ: Fraction who die of natural causes • λ: Numbers of pathogen shed per infectious/asymptomatic individual • β0 : Baseline transmission rate • β : Infection rate due to pathogen Dynamic Modeling of Disease Transmission: an example dX dt a gZ X 0 X (W ) X Remember: a derivative is a rate of change X= the population of individuals susceptible to a disease dX/dt = rate of change in the susceptible population The equation describes individuals moving in and out of the susceptible population Each variable represents some number of individuals moving into the susceptible population (+) from some other group, out of the susceptible population (-) to some other group Dynamic Modeling of Disease Transmission: an example dX dt a gZ X 0 X (W ) X a= number of susceptible individuals migrating into the population γZ =number of non-infectious/asymptomatic individuals migrating back into the susceptible population μX =Fraction of susceptible individuals who drop out of the susceptible population because they die of natural causes β0X =number of susceptible individuals who become infected and drop out of the susceptible population β(W)X =number of susceptible people becoming ill due to pathogen exposure and drop out of the susceptible population Analysis of Disease Transmission Models Traditional approaches to evaluating dynamics models are qualitative – Stability analysis, threshold estimates (Ro), qualitative fits – Statistics rarely used to analyze output Methodological goal to obtain public health relevant estimates of the outbreak – Need to modify traditional statistical techniques to address models with large number of parameters, sparse data, and collinearity Analysis of Disease Transmission Models Likelihood Traditional likelihood methods – Difficult to find maximum likelihood point in highly parameterized models. – Confidence intervals are often not possible in complex likelihood spaces Profile likelihood is an alternative option – Fix a subset of the parameters across a grid of values. – At each point in the grid the remaining parameters are maximized. Bayesian techniques Practical for combining outbreak data with existing information about parameters. Modifications required to deal with collinearities Model 1 Goals: To examine the role of person-person (secondary) transmission To estimate the fraction of outbreak cases associated with person-person (secondary) transmission Cryptosporidium Outbreak - Model Diagram IA(t) r S(t) Susceptible + S E1 p E2 p ... p Ek Latently Infected Infectious (asymptomatic) p d 1r IS(t) Infectious (symptomatic) W(t) Environmental Transmission S: Susceptible W: Concentration of Pathogens in the Environment IS: Symptomatic and Infectious IA: Asymptomatic and Infectious R: Immune/ Partially Protected Solid: Individual Flows from State to State Dashed: Pathogen Flows R(t) Removed Analysis - Model 1 Monte Carlo Markov Chain (MCMC) was used to generate a posterior distribution. Two step procedure was used to address collinearities of the parameter estimates – – MCMC at profiled points Second MCMC on draws from first MCMC Cumulative incidence, I1, was produced by a random draw of the posterior Cumulative incidence, I0, was produced by first setting bs=0 then obtaining a random draw of the posterior. The attributable risk associated with secondary transmission was I1- I0 Risk Attributable to Secondary Transmission 10% , 95% CI [6, 21] 700 600 Frequency 500 400 300 200 100 0 0 0.1 0.2 0.3 Percent attributable risk 0.4 0.5 Model 2 Goal: To examine the role of person-environmentperson transmission To estimate the preventable fraction due to an increase in distance between wastewater outlet and drinking water inlet Examine preventable fraction as a function of transport time parameter, d – Where d is a surrogate for the potential intervention of moving the drinking water inlet farther from the wastewater outlet Cryptosporidium Outbreak- Model Diagram IA(t) r S(t) Susceptible + S E1 p E2 p ... p Ek Latently Infected Infectious (asymptomatic) p d 1r IS(t) R(t) Removed Infectious (symptomatic) W(t) Environmental Transmission S: Susceptible W: Concentration of Pathogens in the Environment IS: Symptomatic and Infectious IA: Asymptomatic and Infectious R: Immune/ Partially Protected Solid: Individual Flows from State to State Dashed: Pathogen Flows Analysis - Model 2 Estimate the likelihood for different values of d, ranging from 1 - 40 days. Estimate the attack rate (AR) for the MLE parameters Estimate the AR for different values of d, keeping all other parameters constant at their MLE values. Plot PFd = 1 - ARMLE / ARd Profile Likelihood of the Delay Parameter MLE for the time between contamination of sewage and exposure from drinking water tap was 11 days (95% CI [8.3, 19]) -2450 Log Likelihood -2455 -2460 -2465 -2470 -2475 -2480 0 5 10 15 20 Days 25 30 35 40 Preventable Fraction As a Function of Delay Time Predicting the public health benefits of moving the drinking water inlet 0.9 Preventable Fraction 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 0 5 10 15 20 25 Days 30 35 40 45 Conclusions Secondary transmission was small. – Best guess is 10%, most likely less than 21% – Consistent with empirical findings of McKenzie et al. – Kinetics of the outbreak in Milwaukee were too quick to be driven solely by secondary transmission Conclusions Person-water-person transmission as the main infection pathway has not been well studied – Few data exist that examines person-waterperson transmission – Studies have demonstrated a correlation between cases of specific viral serotypes in humans and in sewage – Provides information on a potentially important environmental intervention Conclusions: Methods Analyzing disease transmission models using statistical techniques Allows inferences about parameters that are interesting and relevant – Can get at posterior distribution that allows for calculation of relevant public health measures Requires the modification of existing techniques – Profile likelihood to deal with large numbers of parameters – Bayesian estimation techniques to address the colinearity. Conclusions Risk assessments should use models that can integrate relevant information Health data – Epidemiology – Basic biology Environmental data – Water quality – Fate and transport Need a population perspective – Model-based approach