Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Typhoid fever wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Trichinosis wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Brucellosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Gastroenteritis wikipedia , lookup
Hepatitis C wikipedia , lookup
Chagas disease wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Tuberculosis wikipedia , lookup
Leptospirosis wikipedia , lookup
Schistosomiasis wikipedia , lookup
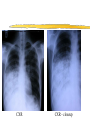
Sumatran Surprise An Intriguing Indonesian Infectious Diseases Dr. M. Wansborough-Jones firm Kathryn Brain Norzehan Hj Md Saini Jeremy Rampling Nikunj Shah MR. A 26 years old, Indonesian, male 8 years in the U.K Speaks little English Delivery man at a takeaway in Battersea PC Productive cough Lymphadenopathy Weight loss Swollen left knee HPC 1 month Hx of productive cough, grey sputum, worse in last 2 weeks, associated SOB An episode of haemoptysis, last Easter, more than a spoonful of blood mixed with mucus 2 weeks ago - fever, shivering, night sweat, took paracetamol, resolved spontaneously HPC cont. Post-prandial nausea, vomited food eaten 2 weeks ago but has good appetite Weight loss (how much, since when?) 1 month Hx of general malaise Occasional headache with vertigo after walking a certain distance, last incident a week ago, had to keep his head up to prevent from fainting, passed out once few months before developed cough HPC cont. SOB on exertion Lumps in neck for a year, submandibular and on both sides, in size, went to see his GP in Jan 2003 & was referred to CIU but failed to turn up for appointments few times Swelling of left knee with lesion & sinus discharging occasionally below the left knee for 3 months, tender and painful to move, lost balance as a result, pain has been there for a year SE No palpitations, central chest pain, oedema No neck stiffness, photophobia No fits, numbness, pins and needles, muscle pain No genitourinary symptoms No other GI symptoms PMH No significant illnesses Vaccinated for BCG but no scar found DRUG Hx Nil No known allergies FAMILY Hx Nil SOCIAL Hx Came to the U.K IN 1994 Went to Saudi Arabia for a month in 97’ Went back to Indonesia for 2 months in 98’ Both parents and two younger sisters in Indonesia - fit and well Lives in 4 bedrooms detached house in Tooting with 3 other people, all fit and well Works as delivery man in an Indian takeaway Social Hx cont. Occasional smoker and drinker Single Never been in any sexual relationship Denies any i.v drug use Physical examination Cachectic, looking unwell No pallor, jaundice, clubbing, cyanosis, koilonychia Temp. - 37.1 °C Sat. - 98% on air Lymph nodes enlargement submandibular and submental, several in anterior cervical chain and a single LN in left axilla Physical examination cont. CVS Pulse - 130 bpm BP - 106/80 mm Hg HS - I + II + 0 Respiratory Right lower zone - dull on percussion, harsh bronchial breathing Crackles on the left base Physical examination cont. Bowel Soft, non-tender, normal bowel sound, No organomegaly CNS Grossly intact Physical examination cont. Left knee - fluctuant swelling + sinus below the knee (dry) Differential diagnosis TB (Post-primary > Primary) Lymphoma Carcinoma of the lung Atypical pneumonia Ix at admission 13/5 FBC (including CRP) U&E LFT Blood culture Sputum microscopy (AFB) Swab from leg CXR Blood results Hb 11.8 WBC 7.9 Neut 6.7 Platelets 240 MCV 77* Na+ 133* K+ 4.9 Urea 5.9 Creatinine 90 Glucose 5.3 CRP 144.5* CXR- R lobar consolidation Bilirubin 9 ALT 42 ALP 92 Albumin 25* Gamma GT 34 Adj Ca2+ 2.25 PO4 1.24 Admitted 13/5 Iv hydration Erythromycin po 500g qds Cefotaxime iv 1g bds CXR CXR - closeup The following day... Ix X ray left knee FNA submental + submandibular lymph nodes TB blood cultures Management Ibuprofen po 400mg tds Knee Knee - closeup 15/5 BINGO!!! Microscopy- AFB positive Legionella/ pneumococcal antigen not detected DIAGNOSIS- Tuberculosis - pneumonia and osteomyelitis Ziehl-Nielsen Stain Bannister, Begg & Gillespie (2000) Anti-TB therapy begins15/5 12 months course Rifater 4 tablets daily (Rifampicin; Isoniazid; Pyrazinamide) Ethambutol 700 mg po od Paracetamol 1g po (QDS max) as required 15/5 Contact tracing Close family members and work colleagues If unwell => rigorous TB Ix If well, CXR and tuberculin test Adult=>CXR; children=> tuberculin Isoniazid prophylaxis if suggestive, or if <1 y.o. Epidemiology Leading infectious cause of death world wide. Increasing in the far east and Africa especially in association with AIDS. Increasing in London and the UK 40x more likely to have in lifetime if of Asian origin. Pathology Infection with Mycobacterium tuberculosis. Mainly in upper of lobe of lungs. Initial infection in childhood, primary infection. This heals and becomes calcified. Reactivation when host becomes immunosuppressed. Manifestations Miliary TB acute diffuse dissemination of tubercle bacilli via the blood stream. Presents very non specifically, weight loss ill health fever. Mantoux test is normally +ve though can be -ve in severe disease. Adult post primary pulmonary TB General onset of non specific symptoms. Main features fever, cough, weight loss. Sputum mucoid, purulent or blood stained. Pleural effusion or pneumonia. Finger clubbing is present with advanced disease. Investigations Chest X-Ray patchy nodular shadows in upper zone. Staining Ziehl-Nielson culture takes 4-8 weeks. Bronchoscopy if no sputum. Biopsy of lymph nodes. Direct testing for rapid result using PCR. Management Sensitive organisms use. Rifampicin, S/E inducer of liver enzymes, should be stopped if bilirubin is elevated. Isoniazid, can cause a polyneuropathy at high doses. Can cause nausea and vomiting. Pyrazinamide reduces renal excretion of urate and an precipitate hyperuraemic gout. Can cause hepatotoxicity. If resistant use ethambutol or myambutol. These can cause optic retro bulbar neuritis. All patients must be seen by an ophthalmologist prior to treatment. Control and prevention TB is a notifiable disease. All close contacts are screened with a mantoux test and a chest X-Ray. Prevention is with immunisation with BCG vaccination administered at 12-13 in the UK Administered at birth to groups at high risk