Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Botulism
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Angela Houston
Dr Angela Houston is a specialist registrar in Infectious Diseases,
Microbiology and Virology in London/ South Coast.
This session provides an overview of botulism. Clinical
presentation, differential diagnosis, treatment and
prevention.
Edited by Prof Tom Solomon and Dr Agam Jung
Learning Objectives
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
By the end of this session you will be able to:
• State the impact of botulism worldwide, microbiology and
transmission
• Describe the actions of botulinum toxin
• Recognise the clinical presentation of botulism and
differential diagnosis
• Specify the laboratory and clinical diagnosis of botulism
• Explain the treatment of botulism
Overview
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
In this session you will learn about the neurological
presentation of botulism.
You will learn about the microbiology, routes of transmission,
presentation, treatment and prevention of botulism and
infections caused by bacterial neurotoxins.
Botulism Microbiology I
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
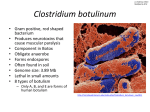
Botulism is a rare and potentially fatal disease caused by a
highly potent neurotoxin released by the anaerobic spore
forming bacterium Clostridium botulinum and, rarely by
Clostridium baratii and Clostridium butyricum.
There are seven neurotoxins (A-G). Illness in humans is
usually caused by types A, B or E, or rarely by F. All toxins
block the release of acetylcholine at the neuromuscular
junction and produce the same neurological syndrome.
Clostridium botulinum is present in the soil and environment
and is responsible for three naturally occurring forms of
botulism, all of which present with the same neurological
features but depend on mode of acquisition.
Botulism Microbiology II
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Clostridium botulinum – CDC Public Health Image Library
#2107
Transmission
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Botulism can be transferred by:
•
•
•
Food-borne from ingestion of contaminated
food with preformed toxin
Infantile botulism caused by ingestion of
spores which colonise the gastrointestinal
tract and produce toxin in vivo
Wound botulism caused by infection of a
wound with Clostridium botulinum and
production of toxin in vivo
There is also a further possibility that botulism
may occur as a result of deliberate release or as
accidental exposure following miss-injection of
therapeutic neurotoxin.
The neurological syndrome produces acute,
symmetrical descending flaccid paralysis.
Types: Food-borne Botulism
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Food-born botulism occurs from ingestion of preformed toxin present
in food which has been stored in airtight (anaerobic) conditions.
Cases have mainly occurred in sporadic outbreaks and the Health
Protection Agency (HPA) reports 33 cases in the UK between 19802006 of which there were three fatalities.
Recent cases have occurred amongst Polish immigrants who eat
home preserved sausages and pickles stored in jars.
Very rarely, intestinal colonisation similar to infant botulism occurs in
adults, usually with an underlying reason, such as gastrointestinal
abnormalities.
Prodromal symptoms begin within hours of ingesting the preformed
toxin.
Types: Infantile Botulism
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Gastrointestinal colonisation occurs when babies ingest
environmental spores of Clostridium botulinum which germinate
within the gastrointestinal tract producing in vivo toxin production.
Babies present anytime from 1 week to 12 months of age (usually <
6 months) with non specific symptoms including:
•
•
•
•
•
•
•
•
Weakness
Hypotonia
Hyporeflexia
Bulbar palsies
Constipation
Poor feeding
Dehydration
Disease progression in children can be very rapid. The disease
presentation is variable and is likely to reflect the differences in
bacterial load and host immunity in infants of different ages.
Only six infantile cases have been reported to the HPA from 19752006 with no fatalities.
Types: Wound Botulism
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Wound botulism was first described in the USA in the 1950s but the
last decade has seen a huge increase in the number of cases and
now is the most common form of botulism seen in the developed
world.
163 cases have been reported to the HPA in the UK from 2000-2009
reflecting the increase in intravenous drug use (IVDU).
The disease is seen almost exclusively in injecting heroin users who
use 'skin popping' as a route of drug administration.
Types: Drug Use
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Heroin used in the UK originates predominantly from Asia and
arrives as a powder which has undergone a number of processing
steps including 'cutting' with bulking agents en route. Any of these
stages may result in the accidental introduction of clostridium
botulinum spores from contaminated material.
In order to inject the drug, it is mixed with an acid usually citric acid
and heated briefly. In IVDUs with limited venous access the material
is injected directly into the skin or muscle ('skin popping'). The acid
results in local necrosis which produces anaerobic conditions ideal
for germination of Clostridium botulinum and toxin production.
It is not seen in IVDUs who inject
directly into veins as the spores
do not have time to germinate in
anaerobic conditions.
Actions of Botulinum
Neurotoxin I
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Regardless of mode of entry
to the human body, the
neurotoxin disseminates
widely in throughout the
vascular system and binds
irreversibly to the
presynaptic sides of
peripheral cholinergic
synapses at ganglia and
neuromuscular junction.
Actions of Botulinum
Neurotoxin II
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
The heavy chain of the toxin binds to the receptors, allowing the
light chain to translocate into the nerve cell via receptor
mediated-endocytosis.
Inside the cytoplasm, the toxin produces an irreversible
disruption in stimulation-induced acetylcholine release by that
presynaptic nerve terminal.
Recovery
Recovery is slow as new synaptic terminals must form from the
original nerve plate, a process that takes approximately six
months.
Adrenergic nerves are unaffected and the toxin seems unable
to cross the blood brain barrier so limiting damage to the
peripheral cholinergic system. If onset is very rapid, there may
be no symptoms before sudden respiratory paralysis occurs.
Clinical Presentation of
Botulism
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Presentation
Adults patients infected with the botulinum neurotoxin
present with similar clinical features irrespective of mode
of acquisition:
• Bilateral cranial nerve palsies
• Descending flaccid paralysis
• Blurred or double vision
• Dysphagia and a dry mouth (often the first
complaints) progressing to a symmetrical flaccid
paralysis and respiratory failure
Differential Diagnosis I
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
The following are diseases with similar clinical features
to botulism:
• Botulism
• Guillain–Barre syndrome (GBS)
• Miller Fisher variant of GBS
• Myasthenia gravis
• Viral encephalitides
• Tick paralysis
• Paralytic shellfish poisoning
• Rabies
Differential Diagnosis II
Botulism
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
•
•
•
•
•
Acute bilateral cranial neuropathies and symmetrical
descending weakness
No fever unless intercurrent infection
Only sensory deficit may be blurred vision
History of exposure – ingestion
IDU or a traumatic wound
Guillain-Barre syndrome (GBS)
•
•
•
•
•
•
Antecedent febrile illness
Ascending symmetrical paralysis
Loss of sensation, parasthesia, pain, loss of reflexes
Electromyograph may help differentiate
Antiganglioside antibody may be elevated in CSF or serum
with GBS or Miller Fisher
No augmentation of modified action potential with repetitive
nerve stimulation at 20-50 Hz in contrast to botulism
Differential Diagnosis III
Miller Fisher variant of GBS
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
•
•
•
•
Antecedent febrile illness
Ascending paralysis and parasthaesia
Early loss of reflexes
Internal and external opthalmoplegia with ataxia which is
more marked than limb weakness
Myasthenia gravis
•
•
•
•
•
•
•
•
Muscular fatigability
Resolution of paralysis with Tensilon (but some improvement
seen in some cases of botulism)
Recurrent paralysis
Sustained response to anticholinesterase therapy
Spinal/paralytic poliomyelitis, almost never sensory loss
Antecedent febrile illness, asymmetrical paralysis
Altered CSF
Meningeal irritation
Differential Diagnosis IV
Viral encephalitides
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
•
•
•
•
•
•
•
Fever and altered mental state
Abnormal CSF
Asymmetric weakness
EEG findings
Cerebrovascular accident
Sensory deficits
Asymmetric hyperactive deep tendon reflexes
Tick paralysis
•
•
•
•
•
•
•
Travel to endemic area (Australia, USA)
Presence of femal tick, may be hidden in long hair
Parasthesia of affected extremities
Ascending paralysis
Loss of deep tendon reflexes
Rare cranial nerve involvement
Occasional cerebellar ataxia
Differential Diagnosis V
Paralytic shellfish poisoning
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
•
•
•
•
•
•
History of consumption of shellfish (or rarely fish)
Incubation of 1 hour
Numbness of face and lips
Parasthesis
Normal reflexes
Respiratory paralysis
Rabies
•
•
•
•
•
Not necessarily following a recent bite
Can be months
Ascending paralysis
Incoordination
Pharyngeal spasm particularly on drinking buy not due to a
breeze of air
Laboratory and Clinical
Diagnosis of Botulism I
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Diagnosis
The diagnosis of botulism is based on clinical suspicion.
Learning Bite: Always seek advise from an
Infectious diseases specialist and ITU.
Demonstration of the toxin in serum can be helpful.
Laboratory and Clinical
Diagnosis of Botulism II
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Food-borne botulism
• In food-borne botulism, toxin is present in serum or
faeces in >50% of cases within one day of onset, but
<25% after 3 days
• C. botulinum will be present in the faeces for longer
which may be helpful diagnostically
• Toxin can be isolated in faecal samples in >70% of
cases within 2 days and 40% 10 days after onset of
food poisoning
Laboratory and Clinical
Diagnosis of Botulism III
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Wound botulism
• In wound botulism, toxin is isolated in the blood in
40% of suspected cases
• It is important to very carefully examine patients for
wounds that may need debridement no matter how
small
• Toxin detection requires 10ml serum sample (ideally
before any antitoxin is administered). This is
measured by a bioassay in mice. The presence of
toxin confirms the clinical diagnosis
• Serum samples are not so helpful in infantile botulism
The Treatment of Botulism I
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Treatment of botulism should include:
•
•
•
•
Early administration of botulinum antitoxin (if indicated)
Search for and debride any wound no matter how trivial
Give antibiotics if wound present
Supportive treatment
The Treatment of Botulism II
Antitioxin
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Antitoxin is an effective treatment and will prevent further
progression of symptoms but will not reverse established
paralysis.
•If administered early it may neutralise any
circulating toxin
•There are a number of antitoxin products available
all of which have been derived from pooled animal
immunoglobulin
•If the patient continues to deteriorate the dose may
be repeated within 24 hours
•Since antitoxin is derived from animal
immunoglobulin it carries a risk of allergic reactions
such as anaphylaxis and serum sickness
The Treatment of Botulism III
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
With antitoxin and good supportive treatment, recovery is
to be expected although it may take weeks or months, so
prolonged hospital admissions are likely.
Learning Bite: Any case of suspected Botulism should
be reported promptly to the HPA.
Key Points
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
•
Botulism is a rare but potentially life threatening disease
caused by neurotoxins of Clostridium botulinum
•
Three endogenous forms exist. Food-bourne, infantile and
wound botulism which is now the commonest form seen with
the rise in intravenous drug users
•
Botulinum toxin binds irreversibly to the presynaptic
membrane at the motor endplate inhibiting release of
acetylcholeine
•
Classically presents with bilateral cranial nerve palsies and an
acute, symmetrical, descending flaccid paralysis in the
absence of fever or cognitive disturbance
•
Diagnosis is clinical but can be aided by identifying Botulinum
toxin in serum or stool samples
•
Treatment is supportive and antitoxin can be effective in
preventing further progression if given early. Wounds infected
with C. Botulinum need urgent debridement and antibiotic
treatment
Summary
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Having completed this session you will now be able to:
• State the impact of botulism worldwide, microbiology and
transmission
• Describe the actions of botulinum toxin
• Recognise the clinical presentation of botulism and
differential diagnosis
• Specify the laboratory and clinical diagnosis of botulism
• Explain the treatment of botulism
References and further reading
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
•
Montecucco, C. and G. Schiavo, Mechanism of action of tetanus and
botulinum neurotoxins. Molecular microbiology, 1994. 13(1): p. 1-8.
•
Brett, M., G. Hallas, and O. Mpamugo, Wound botulism in the UK and
Ireland. Journal of medical microbiology, 2004. 53(6): p. 555.
•
Cherington, M. Botulism: update and review. 2004: [New York]:
Thieme-Stratton Inc.,[c1981].
•
McLauchlin, J., K. Grant, and C. Little, Food-borne botulism in the
United Kingdom. Journal of Public Health, 2006. 28(4): p. 337.
•
Lindstrom, M. and H. Korkeala, Laboratory diagnostics of botulism.
Clinical microbiology reviews, 2006. 19(2): p. 298.
•
Bleck, TP. Clostridium botulinum (botulism). In: Principles and Practice
of Infectious Diseases, 6th ed. Mandell, GL, Bennett, JE, Dolin, R,
(Eds), Churchill Livingstone, Philadelphia, PA 2005, p. 2822.
•
Health Protection Agency Website.
•
Antitoxin and advice are available from the duty doctor at the Health
Protection Agency, Centre for infections in the UK. For infant botulism a
human derived Botulinum immune Globulin BabyBIG® is available
from the Infant Botulism Treatment and Prevention Program (IBTPP)
California USA.
Question 1
BOTULISM
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Learning Objectives
Overview
Microbiology
Transmission
Types of Botulism
Actions of the toxin
Clinical features
Differential
diagnosis
Investigations
Treatment
Key points
Summary
References and
further reading
Questions
Which of the statements are correct with regards to the
botulinum toxin?
a) Botulinum toxin is one of the most potent neurotoxins known
b) Botulism is most commonly caused by the Botulinum
neurotoxins A and C
c) Causes inhibition of the action of GABA
d) Affects the peripheral and central nervous system