Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cryptosporidiosis wikipedia , lookup
Trichinosis wikipedia , lookup
Henipavirus wikipedia , lookup
West Nile fever wikipedia , lookup
Schistosomiasis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Marburg virus disease wikipedia , lookup
Neonatal infection wikipedia , lookup
Hepatitis C wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Herpes simplex virus wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Epidemiology of HIV/AIDS wikipedia , lookup
Hepatitis B wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
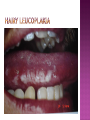
BY DR MAHESH MATHUR,MD,DCP DERMATOLOGIST CMS WHY SHOULD WE KNOW ABOUT THIS DISEASE ? In July 1981 – Birth Year of HIV/AIDS -Lawrence Altman in the New York times Dec.1982 Epidemic in MSM In 1984 –The Agent- retrovirus-HTLV III Renamed in 1986 HIV & serological tests In 1987 –Zidovudine Since 1996- HAART –Dramatic decrease in Mortality 41 million people are infected with HIV world wide (UNAIDS) >70% Reside in Sub- Saharan Africa; App. 16000 New infection occurs Daily, Majority Young adults. HIV is Leading single cause of Death in young. 500 Young adults & 1000 Children dieing every day Millions Estimated number people living with HIV in Asia, 1990–2007 7 6 5 4 3 2 1 0 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 20062007 Year This bar indicates the range HIV-1 and the less common HIV-2 belong to the lentivirus group of virus of the family retroviruse. HIV-1 contains a single-stranded RNA genome -9 genes that encode 15 different proteins. The major viral proteins are structural proteins (Gag, Pol, and Env), Regulatory proteins (Tat and Rev), Accessory proteins (Vpu, Vpr, Vif, and Nef). Three major classes of HIV-1 M (main), 90% N (new), and O (outlier). -gp120 -gp 41 -P24 Three components of the host-virus interaction. The virus itself - Viral strains lacking nef sequences do not produce AIDS in their hosts.(Australian cohort) Innate host factors are important in containing infection. CCR5,CXCR4 the "second receptor" on CD4 T cells The humoral and cellular arms of immune system . Humoral responses -detectable one to six months following infection. The viremia of acute infection is controlled by cytotoxic T lymphocytes Cellular immunity CD4 helper T cells. The characteristic quantitative & qualitative depletion of CD4+ T lymphocytes in HIV, Cellular destruction, Diminished cellular production, Cellular sequestration in lymphoid organs CD8 T lymphocytes (CTLs)- kill HIVinfected cells - immune mechanism regulating HIV replication SEXUAL CONTACT–53% PERINATAL TRANSISSION –15 to 40 % HOMO & HETERO SEXUAL CONTACT TRANS PLACENTAL 70% of infection DURING DELIVERY THROUGH INFECTED BIRTH CANAL 10 to 15 % AS A RESULT OF INGESTION OF BREAST MILK CARRYING VIRUS 15% TRANSFUSION OF BLOOD,BLOOD PRODUCTS & ORGEN DONATION CONTAMINATED NEEDLES HEALTHCARE WORKERS HAVE A RISK OF APP. 0.3% FOLLOWING A SINGLE NEEDLE-STICK INJURY WITH KNOWN HIV INFECTED BLOOD ACCIDENTAL INOCULATION ~0.09% CLINICAL CATEGORIES A – ADULT/ADOLESENT >13 YEARS WITH DOCUMENTED HIV INFECTION & CONDITIONS LISTED IN B&C NOT PRESENT B – CONDITIONS ATTRIBUTED TO HIV INFECTION ORINDICATIVE OF DEFECT IN CMI AND PHYSICINE CONSIDERING HIV INFECTION IN MANAGEMENT OF DISEASES C- AIDS DEFINING CONDITIONS PGL/ACUTE SEROCON VERSION HIV RELATED CONDITION AIDS CASE DEFINITION A1 B1 C1 200-499 A2 B2 C2 <200 A3 B3 C3 ABSOLUTE CD 4 COUNT >500/mm3 He or she has a CD4+ cell count <200 cells/µL, or His or her CD4+ cells account for <14% of all lymphocytes, or That person has been diagnosed with one or more of the AIDS-defining illnesses listed below. MUCOCUTANEOUS LESIONS Cutaneous infection associated with HIV/AIDS Viral- HSV, VzV, Molluscum Contagiosum Bacterial – Staphylococcus, Bacillary Angiomatosis,Mycobacteria Fungal – Candidia,Dermatophytosis Penicillium Parasitic infection - Scabies Inflammatory Non infectious Dermatosis Eosinophilic Folliculitis Seborrheic Dermatitis Pruritus psoriasis Adverse Cutaneous Drug eruptions HIV & Skin Cancers -Screen blood -Diagnose infection, -Monitor disease progression in individuals infected by HIV. 1) Detect antibody, 2) Identify antigen, 3) Detect or monitor viral nucleic acids, and 4) Estimate of CD 4 +T-lymphocyte - ELISA TEST FOR HIV-1 & 2 (gp120,41) >99.5% SENSITVITY FALSE POSITIVE OCCURS IN HEPATIC DISEASE ACUTE VIRAL INFECTIN RECENT VIRAL VACCINATION AUTOANTBODIES The p24 antigen assay The viral (core) p24 protein in blood, Detectable earlier than HIV antibody during acute infection. -Highly specific with high levels of viremia during which the individual is highly infectious. PCR - 99.9%. Testing is of value in: -detecting early HIV infection, -screening blood, -diagnosing infection in the newborn, -monitoring antiviral therapy. - VIRAL RNA TEST RT-PCR bDNA NASBA Where it has succeeded, Highly Active Antiretroviral Therapy (HAART)has altered the nature of HIV disease, Transforming an almost uniformly fatal illness into a chronic but apparently stable tratable condition. There are currently 5 major classes of antiretroviral drugs in general use: Nucleoside analogue reverse transcriptase inhibitors (NRTIs), Nonnucleoside reverse transcriptase inhibitors (NNRTIs), Protease inhibitors (PIs), Fusion inhibitors. Integrase Inhibitors NRTIs -Inhibit the synthesis of DNA by reverse transcriptase, enzyme that copies viral RNA into DNA in the newly infected cell. Reverse transcriptase fails to distinguish the phosphorylated NRTIs from their natural counterparts & use the drugs in the synthesis of viral DNA. When an NRTI is incorporated into a strand of DNA being synthesized, the addition of further nucleotides is prevented, and a fulllength copy of the viral DNA is not produced. ZIDOVUDIN,DIDANSINE,LAMIVUDIN ZALCITABIN NNRTIs also inhibit the synthesis of viral DNA, but rather than acting as false nucleotides, the NNRTIs bind to reverse transcriptase in a way that inhibits the enzyme's activity. DELAVIRDINE,EFAVIRENZ,NEVIRAPIN PIs bind to the active site of the viral protease enzyme, preventing the processing of viral proteins into functional forms. Viral particles are still produced when the protease is inhibited, but these particles are ineffective at infecting new cells. INDINAVIR,RITONAVIRNELFINAVIR Fusion inhibitors prevent HIV from entering target cells. Drugs of this class bind to the HIV envelope protein gp41, which is involved in viral entry. By blocking the interactions between regions of the gp41 molecule, fusion inhibitors interfere with the conformational change (folding) of the envelope molecule required for fusion with the target cell membrane. ENFUVITIDE SYMPTOMATIC HIV INFECTION ANY CD4 COUNT/VIRAL LOAD TREAT ESTABLISHED AIDS CD4 <200 TREAT ASYMTOMATIC INFECTION CD4 – 201TO350 >350 (2NRTIS+NNRTS OR 2NRTIS+PI OR 3NRTIS) ANY VIRAL LOAD CONSIDER TREATMENT ON VIRAL LOAD,CD4 DECLINING CLINICAL CONDITION DEFER TREATMENT Nucleoside/Nucleotide Analogues HYPERSNSITIVITY REACTION SKIN RASHES & SKIN PIGMENTATION MITOCHONDRIAL DYSFUNCTION & LACTIC ACIDOSIS MEGALOBLASTIC ANEMIA & MYELOSUPPRESSION POLYNEUROPATHY WITH ZALCITABIN NAIL PIGMENTATION WITH ZUDOVUDIN Nonnucleoside Reverse Transcriptase Inhibitors SKIN RASHES, SJ SYNDROME HEPATOTOXICITY CONTRAINDICATED IN PREGNANCY PROTEASE INHIBITORS ABNORMAL LIVER FUNCTION BODY FAT REDISTRIBUTION ABNORMAL PLASMA LIPIDS HYPERGLYCEMIA & PANCREATITIS WITH RITONAVIR & SQUINAVIR NEPHROLITHISIS WITH INDINAVIR The protection against exposure to HIV. Antiretroviral therapy cannot replace behaviours that help avoid HIV exposure sexual abstinence, sex only in a mutually monogamous relationship with a noninfected partner, consistent and correct condom use, abstinence from injection-drug use, consistent use of sterile equipment by those unable to cease injection-drug use). Medical treatment after sexual, injection-drug-use, or other nonoccupational HIV exposure is less effective than preventing HIV infection by avoiding exposure Non occupational exposure Any direct mucosal, percutaneous, or intravenous contact with potentially infectious body fluids that occurs outside perinatal or occupational situations e.g., health-care, sanitation, public safety, or laboratory employment. Potentially infectious body fluids are blood, semen, vaginal secretions, rectal secretions, breast milk or other body fluid that is contaminated with visible blood Antiretroviral therapy initiated as soon as possible within 48--72 hours of sexual, injectiondrug--use, and other substantial nonoccupational HIV exposure Recommendations for the prompt initiation of nPEP with HAART when persons seek care within 72 hours after exposure, The source is known to be HIV infected, and the exposure event presents a substantial risk for transmission. When the HIV status of the source is not known and the patient seeks care within 72 hours after exposure, PEP in not recommended for Kissing & other sexual contact without semen/blood mucosal contact The diminished potential benefit of nPEP outweighs the potential risk for adverse events from antiretroviral medications. Health workers -Doctors, Dental surgeons,Nurses,lab worker etc. Percutaneous nedlestick, deep injury,mucosal contact or dameged skin with blood/fluids with high viral load Contact of mucosa with other fluids with high viral load Transmission is 0.3% before ART HAART for 4 weeks is recommendade Follow up is essential EDUCATION COUNSELING BEHAVIOR SAFER MODIFICATION – SEX MONOGAMOUS BE GOOD BOYS & GIRLS