Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
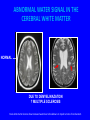
NEURO IMAGING Dr. Francis Neuffer Department of Radiology USC-SOM GOALS AND OBJECTIVES • Review major imaging modalities of neuro imaging. CT, MR, Ultrasound, Angiography • Review classic disease states of vascular, traumatic, infectious and neoplastic diseases. DIGITAL SCOUT FILM SHOWING BEGINNING AND END OF CT SCAN. Multiple sectional images are obtained from a preliminary scout image showing the beginning and end of the scan. iV Contrast enhancementNON-CONTRAST STUDY IV IODINE CONTRAST STUDY ANATOMY Selected images from CT scans posterior fossa level Basilar Artery Supracellar Cistern Temporal Horn lateral ventricle 4th Ventricle Pons Cerebellum ANATOMY Thalamic level 3rd ventricle Sylvian fissure Atria Lateral Ventricle Thalamus Falx cerebri ANATOMY Internal capsule level Anterior Horn Lateral ventricle Caudate Nucleus Internal capsule Lentiform nucleus Occipital Lobe ANATOMY Ventricle level Anterior Horn Lateral ventricle Posteror Horn Lateral ventricle ANATOMY Lateral ventricle level Frontal lobe Body lateral ventricle Parietal lobe Occipital lobe Falx cerebri ANATOMY Supraventricular level Gyrus Centrum Semiovale Sulcus Superior Sagittal Sinus MAGNETIC RESONANCE • Hydrogen protons align in magnetic field • Radio frequency(RF) excitation and transmission • No ionizing radiation MR SIGNAL T1 SCAN T2 SCAN SCANS ARE DESIGNED TO SHOW SPECIFIC TISSUE AND SPECIFIC PATHOLOGY VARIOUS MRI SEQUENCES T1 FLAIR (edema) The tissue signal varies depending on the type of scan performed. T2 (CSF/edema) Diffusion NORMAL CEREBRAL ARTERIOGRAM NORMAL ULTRASOUND Flow is seen at the common carotid bifurcation on contrast X- ray arteriography and B-mode ultrasound. CAROTID ARTERY Color Doppler The vessel lumen can be imaged with ultrasound and the velocity of the flow can be measured. A stenotic lesion will show acceleration of flow through the narrowed lumen. Catheter injection of RT common carotid artery ACA MCA ECA ICA CCA • • • • • CCA common carotid A. ICA internal carotid A. ECA external carotid A. MCA middle cerebral A. ACA anterior cerebral A. VASCULAR ANATOMY Images of vessels at the Circle of Willis ACA MCA MR VASCULAR ANATOMY Anterior cerebral Middle cerebral Basilar artery ECA ACA MCA Carotid bulb ICA Vertebral artery CCA ICA MR Angiogram- venous injection Images can be obtained at MR by injecting gadolinium and imaging rapidly as the agent circulates through the arterial circuit. WHO ARE THE PATIENTS ? • VASCULAR ISCHEMIA • TRAUMA • INFECTIOUS WORKUP • MALIGNANCY WORKUP CT SCANNING as initial sorting • Ischemia – Global – Focal Hemorrhage – – – – Hypertensive hemorrhage Amyloid angiopathy Hemorrhagic infarction Subarachnoid hemorhage FOCAL DEFICIT OF 24 HRS • ACUTE CVA 85% ISCHEMIC 15% HEMORRAGHIC • TREATMENT DIFFERENCE ANTICOAGULATION FOR ISCHEMIC CVA STENOSIS NORMAL CT OF ISCHEMIC STROKE 1 DAY POST 2 DAY POST Note increase in edema LACUNAR INFARCT Small vessel = lenticulostriate vessel MCA proximal branch basal ganglia-thalamic VASCULAR DISTRIBUTIONS Anterior Cerebral Artery Middle Cerebral Artery Posterior Cerebral Artery The different vascular distributions of cerebral territories are represented on color coded CT diagrams CT SCANNING as initial sorting Hemorrhage – – – – Hypertensive hemorrhage Amyloid angiopathy Hemorrhagic infarction Subarachnoid hemorhage SUBARACHNOID HEMORHAGE Increased density Normal The supra sellar cistern is white due to the blood mixed with the CSF. SUBARACHNOID HEMORRHAGE • Blood in the subarachnoid space – Between the Pia & Arachnoid – CT – acute blood, increased density – Rupture of cerebral aneurysm • “Worst Headache of Life” • Location: basal cisterns, sylvian fissure, cortical sulci. CAROTID ANEURYSM Associated with Polycystic Renal disease And Marfans Syndrome Aneurysms are often at vascular branch points and show relative deficit of media there which contributes to vessel wall weakness INTRACEREBRAL HEMORHAGE HYPERTENSIVE EVENTS Acute Blood is dense on Non contrast CT Pontine Hemorrhage Thalamic Hemorrhage CEREBRAL AMYLOID ANGIOPATHY (CAA) IS AN IMPORTANT CAUSE OF SPONTANEOUS CORTICALSUBCORTICAL INTRACRANIAL HEMORRHAGE (ICH) IN THE NORMOTENSIVE ELDERLY. Chao C P et al. Radiographics 2006;26:1517-1531 Hemorragic infarction—delayed several days With reperfusion on infarct area there is hemorrhage into infarct zone with local mass effect and midline shift. CT SCANNING as initial sorting • Ischemia Hemorrhage – – – – Hypertensive hemorrhage Amyloid angiopathy Hemorrhagic infarction Subarachnoid hemorhage GOAL FOR IMAGING Comparison of infarct zone and ischemic zone to identify treatment candidates STROKE INTERVENTION • Thrombolytic therapy to salvage ischemic brain at the border of the infarct zone (ischemic penumbra). • Who benefits and how to select? STROKE INTERVENTION • Thrombolytic therapy 3-6 hour window • Risk of hemorrhagic conversion Typically 3hrs since onset is the limit for initiation of venous thrombolytic therapy. With arterial therapy the window of action can be extended . The risk of bleeding into the infarct zone with reperfusion is a complication that can worsen prognosis. Lt Rt Note acute occlusion of Rt. MCA circulation and edema in Rt. hemisphere on CT. Comparison of the normal Lt. side is shown. catheter Catheter is advanced for thrombolysis of the MCA thrombus with improved perfusion on last injection of contrast. CT vs. MR ? Abnormality on CT Questionable lesion on CT in a Rt. periventricular location. Compared to CT--MR scans with T1, T2, and diffusion weighted better show the acute evolving ischemic infarction T1 T2 Diffusion MR vs. CT IN EARLY CVA MR LIMITATIONS • COMPLEX MR SIGNAL OF HEMORRHAGE RELATED TO HEMAGLOBIN—Fe EFFECTS • UNSTABLE PATIENT-PATIENT MOTION MORE A PROBLEM IN MR (LONGER SCAN TIME) • CT READILY VISUALIZES BLOOD PRODUCTS • ACCESS- CT IS AVAILABLE FOR ER PATIENTS CT SCANNING as initial sorting • Ischemia – Global – Focal Hemorrhage – – – – Hypertensive hemorrhage Amyloid angiopathy Hemorrhagic infarction Subarachnoid hemorhage WHO ARE THE PATIENTS? • HEAD TRAUMA SUBDURAL HEMATOMA • Venous bleeding from “bridging veins” which connect cerebral cortex to Dural sinuses • Concave inner margin – Older patient –atrophy enlarged subdural space unstable gait–falls – Pediatric patient –shaken baby/child abuse small subdural space can lead to herniation SUBDURAL HEMATOMA (ACUTE) Over time the blood breaks down and decreases in density. SUBDURAL HEMATOMA Hit head on RT. With superficial scalp hematoma Subdural hematoma on LT due to tearing of bridging veins with Deceleration with fall. FRACTURE EPIDURAL HEMATOMA Cause: laceration of meningeal artery/vein adjacent to inner table. Lucid interval post trauma –later cns injury due to mass effect Epidural hematomas are more focal than subdurals since the blood is more confined by the periosteum of the skull. MIDDLE MENINGEAL ARTERY SKULL BASE FRACTURE Can lead to cerebral spinal fluid leak and risk of meningitis The purple ecchymosis behind the ear is called Battle sign described as a clinical finding “RACCOON EYES” Periorbital ecchymosis is another sign of a basal skull fracture. Blood tracks along the periosteum and can collect in soft tissues of the orbital lid. CSF rhinorhea can occur with fractures extending through cribriform plate CT HEAD TRAUMA AIR IN FRONTAL SINUS FRONTAL LOBE CONTUSION NORMAL CHORIOD PLEXUS CALCIFICATIONS TRAUMATIC PNEUMOCEPHALUS Air extends intracranially from fracture of the skull or through the sinuses. INTRACERBRAL PRESSURE HERNIATION • Tonsillar - brainstem - cardiopulmonary arrest. • Falcine - anterior cingulate gyrus –ACA infarct. • Uncus- temporal lobe-- 3rd nerve WHO ARE THE PATIENTS? • CNS INFECTION MENINGITIS bacterial / viral • • • • Little role for imaging-can delay treatment Lumbar puncture and gram stain Meningococcal Bacterial can be fatal Headache, Stiff neck, Fever, Photophobia SINUSITIS AND EPIDURAL ABSCESS Spread of sinus infection to the epidural space can occur. AIDS PATIENTS • TOXOPLASMOSIS --ring enhancing lesions • • • Atrophy -- HIV viral effect PML -- progressive multifocal leukodystrophy JC virus reactivated-fatal-rapid HIV AND TOXOPLASMOSIS ring enhancing lesions on CT noncontrast contrast Patients with altered immunity are subject to many atypical infections. Toxoplasmosis is rarely seen in immunocompetent patients. WHO ARE THE PATIENTS? • CNS MALIGNANCY • Metastatic disease- 50/50 -Primary malignancy TUMORS • Primary = Metastatic • Lung, Breast, Renal • Adult- Supratentorial primary tumors • Pediatric- Infratentorial primary tumors METASTATIC LESIONS HISTORY / MULTIPLE enhance with contrast The ring enhancing lesion is the site of abnormal blood/brain barrier. The low density center often is necrotic tissue. CT WITH CONTRAST ADULTS Glioblastoma Multiforme • Malignant astrocytoma-supratentorial • Can cross midline -corpus callosum • Butterfly Coronal section GBM Axial section MR with gadolineum contrast MENINGIOMA-benign DURAL BASED LESIONS CAN BE LARGE. INCREASED DENSITY is due to calcium and not bleeding TUMORS • Pediatric- Infratentorial primary tumors PILOCYSTIC ASTROCYTOMA • • • • • Pediatric Benign Cystic with nodule Posterior fossa Cerebellum MEDULLOBLASTOMA • Pediatric-malignant-PNET • Post fossa -cerebellum • Spread via CSF WHO ARE THE PATIENTS? • VISUAL SYMPTOMS Bitemporal hemianopsia • PITUITARY LESIONS• impinge on optic chiasm SKULL MR- BRAIN SELLA NORMAL PITUITARY NORMAL PITUITARY ADENOMA CRANIOPHARYNGIOMA • Rathke’s pouch - grow from mouth to between anterior and posterior pituitary • Bitemporal hemianopsia • Pediatric patient • Calcify-Benign WHO ARE THE PATIENTS? • HEARING LOSS • Conduction vs sensory • Weber and Rinne test SCHWANNOMA INTERNAL AUDITORY MEATUS LESION MR SCANS WITH GADOLINIUM WITHOUT GADOLINIUM Bilateral lesions associated with Neurofibromatosis 2. WHO ARE THE PATIENTS? • CHRONIC NEUROLOGIC SYMPTOMS • DEMENTIA • Alzheimers, Multi infarct, Hydrocephalus NORMAL ATROPHY With Alzheimer’s disease little is seen on MR and CT except atrophy as a nonspecific finding. Coronal scans NORMAL PRESSURE HYDROCEPHALUS Dllated ventricles NORMAL NPH NORMAL PRESSURE HYDROCEPHALUS • • • • • CSF not absorbed by arachnoid granulations Ventricles dilate Stretch fibers around ventricles - corona radiata Incontinence, Gate disturbance and Dementia LP/Shunt improves symptoms WHO ARE THE PATIENTS? • CHRONIC NEUROLOGIC SYMPTOMS • DEMYELINATING DISEASE ABNORMAL WATER SIGNAL IN THE CEREBRAL WHITE MATTER NORMAL DUE TO DEMYELINAZATION ? MULTIPLE SCLEROSIS Focal white matter lesions show increased water due to breakdown on myelin at sites of involvement. DEMYLINATION MULTIPLE SCLEROSIS • • • • • • Autoimmune- northern latitudes Young adult- femaleBlurred vision –optic nerve Internuclear ophthalmoplegia - CN 3 and 6 Sensory deficit Autonomic dysfunction- bladder/bowel IF YOU FEEL LOST THERE’S STILL HOPE CT -acute hemorrhage MR- chronic Ultrasound- vascular screening Angiography- intervention