Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
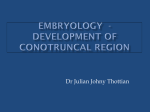
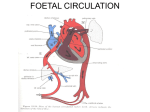
Embryology of the Heart The audio narrations of these slides may have been transcribed verbatim. Check http://www.anat.sunysb.edu/HBA531/Embryology/ to see if they are available for download. For the puposes of narration, this is slide number 0. Cardiogenic area derived from Intra-embryonic mesoderm - mid 3rd week Figures: Sadler 2004 Two cardiogenic cords develop within cardiogenic area. Cords become canalized to give rise to two endocardial heart tubes. Figure: Larsen 1993 Figure: Sadler 2004 Late 3rd week Figures: Sadler 2004 Late 3rd week Figures: Sadler 2004 Figure: Larsen 1993 Endocardial heart tubes come to lie side by side ventral to foregut. Figure: Larsen 1993 •At 21 days, two endocardial heart tubes begin to fuse into one tube. •Caudal end of heart tube in anchored in septum transversum. •Cranial end is developing connections to paired dorsal aortae. •Fusion of tubes is complete by 23 days. Figure: Gilbert 1989 Figure: Moore&Persaud 1998 On day 22, tube begins to elongate, and develops alternate dilations and constrictions. Begin to see primitive heart chambers: •Bulbus cordis •Ventricle •Atrium Figure: Larsen 1993 Truncus arteriosus •On day 23, common venous collection chamber added: sinus •venosus, and common origin for aortic arches: truncus arteriosus. •As heart tubes elongates, loop forms to right: bulboventricular loop. Figures: Sadler 2004 Figure: Larsen 1993 Day 23 By day 22 or 23, contractions of myogenic origin begin. Occur in peristaltic waves beginning at venous end. Figure: Sadler 2004 Day 24 Figure: Sadler 2004 Figure: Moore&Persaud 1998 Figure: Gilbert 1989 Figure: Larsen 1993 4 week heart Figure: Sadler 2004 4 – 5 week heart Figure: Sadler 2004 4 week heart Externally, ventricle and atrium appear to have right and left sides. Figure: Sadler 2004 4 week heart Internally, there is still unidirectional blood flow: Sinus venosus RA LA Atrioventricular Canal LV RV(bulbus cordis) Conus cordis (bulbus cordis) Truncus arteriosus Figure: Gilbert 1989 Late 4th week – swellings develop in dorsal and ventral walls of atrioventricular canal: AV endocardial cushions. Figure: Gilbert 1989 Late 4th week: View from the right side. Figure: Gilbert 1989 Figure: Gilbert 1989 During 5th week endocardial cushions fuse to divide AV canal into right and left AV canals. Figure: Gilbert 1989 Division of atrium into right and left atria also begins in the 5th week. Figure: Gilbert 1989 Division of atrium begins with the appearance of a crescent-shaped membrane that appears in roof and grows ventrally toward the endocardial cushtions: septum primum. Figure: Gilbert 1989 The opening between the growing septum primum and the endocardial cushions, which allows blood flow from right to left, is called the foramen primum. Figure: Gilbert 1989 As septum primum grows, foramen primum gets smaller eventually disappears. New foramen develops high up in septum: foramen secundum. Figure: Gilbert 1989 Toward end of 5th week, new crescent-shaped ridge appears in roof of atrum to right of septum primum: septum secundum. More muscular than first. Figure: Gilbert 1989 As septum secundum grows (into 6th week), covers foramen secundum. Opening made by inferior margin of septum secundum called foramen ovale. Foramen ovale persists throughout fetal development. Figure: Gilbert 1989 Figure: Larsen 1993 Figure: Larsen 1993 Close approximation between opening of inferior vena cava and foramen ovale causes blood from the IVC to pass from RA to LA, and into LV and out aorta. Because septum secundum is rather rigid while septum primum is more flexible, combination of septa and formena work as a unidirectional flutter valve. Figures: Gilbert 1989: Moore&Persaud 1998 As atrium is being divided, part of sinus venosus is drawn Into wall of RA giving rise to smooth-walled portion of RA known as the sinus venarum. Another part of sinus venosus is incorporated into the LA, and gives rise to a pulmonary vein, the stem of which is also drawn into wall of the LA. Figures: Larsen 1993 Figure: Moore&Persaud 1998 Figure: Sadler 2004 Figure: Moore&Persaud 1998 Day 35 Figure: Sadler 2004 Completion of the interventricular septum is problematic because truncus arteriosus is a right sided structure, and blood from LV must pass through IV foramen to exit out the aorta. Figure: Langebartel&Ullrich 1977 If the truncus had been positioned in the midline, then the ventricles could be separated by the spiral septum merging with the original IV septum. Figure: Langebartel&Ullrich 1977 Figure: Langebartel&Ullrich 1977 But since the truncus is on the right, the ventricles are separated by the addition of an oblique septum derived from bulbar ridges, truncal ridges, and endocardial cushions, that partition off part of the bulbus cordis to be incorporated into the LV as the aortic vestibule. To divide the ventricle while maintaining an outflow track for the LV, must divide the bulbus cordis so that part is incorporated into the LV for its outflow track. Figures: FitzGerald 1978 Beginning in 5th week, bulbar ridges (neural crest cells) form in right posterior and left anterior walls of bulbus cordis. Endocardial cusion area also begins to proliferate. Figures: FitzGerald 1978 The septum created By the fused bulbar ridges fuses to the aorticopulmonary septum superiorly. Inferiorly, the bulbar septum joins with original interventricular septum and with material from endocardial cushions to complete division of the ventricle. Figure: FitzGerald 1978 Figure: Sadler 2004 Completion of Interventricular Septum • Original IV septum becomes thick-walled portion of adult IV septum • Part of septum derived from bulbar ridges, truncal ridges and endocardial cushions becomes membranous portion of adult IV septum • Right anterior portion of bulbus cordis incorporated into RV as conus arteriosus or infundibulum • Left posterior portion of bulbus cordis incorporated into LV as aortic vestibule By 8 weeks all major components of heart development are complete • As septa are developing, internal features such a trabeculae carneae within the ventricles are developing • Atrioventricular valves form on R & L • Semilunar valves form in aorta and pulmonary trunk • Conducting system develops Cardiac Malformations • Because development is complex, malformations are relatively common – Approximately 20% of congenital malformations involve heart and/or great arteries – Estimated to occur in about 1% live births and ten times more frequently in still births (Sadler 2004). • Following list are fairly common defects amenable to surgery Atrial Septal Defects (ASD) • Interatrial septum fails to form properly • More common in females than males (3:1) • If large, will cause interatrial shunting of blood and hypertrophy of RV and pulmonary trunk • Large ASD: 6 out of 10,000 births (0.06%) Atrial Septal Defects (ASD) Figure: Moore&Persaud 1998 Atrial Septal Defects (ASD) Incomplete fusion of septum primum and septum secundum large enough for a probe to pass through: Probe patent foramen ovale. Estimated to occur In about 25% of population. Figure: Moore&Persaud 1998 Atrioventricular Septal Defect Figure: Moore&Persaud 1998 Ventricular Septal Defect (VSD) • Interventricular septum incomplete and fails to fully divide ventricles • Most common of all congenital cardiac defects: – About 25% of cardiac abnormalities documented in live births include VSDs – Isolated defects occur in 10-12 of 10,000 births (0.10%) – More common in males than females Normal complete interventricular septum •Most VSD occur in membranous portion of septum •Less commonly, VSD occur in muscular part of septum, probably due to excessive resorption of myocardial tissue Figure: Sadler 2004 Figure: Sadler 2004 Dextrocardia Figure: Moore&Persaud 1998; Larsen 1993 Abnormal Division of Truncus Arteriosus Persistent truncus arteriosus •Failure of aorticopulmonary septum to form •Approximately 1 in 10,000 births (0.01%) •Necessarily includes VSD •Results in mixing of blood from R&L sides of heart •Can be fatal if untreated Figure: Sadler 2004 Abnormal Division of Truncus Arteriosus Transposition of Great Arteries •Aorticopulmonary septum does not spiral •Approx. 2 in 10,000 births (0.02%); more common in infants of diabetic mothers; more common in males than females (3:1) •Usually mixing of blood through patent foramen ovale or ductus arteriosus Figure: Sadler 2004 Abnormal Division of Truncus Arteriosus Unequal Division of Truncus Arteriosus •One artery large, other small (stenotic) •Ventricle on stenotic side must work harder, typically hypertrophies •Often aorticopulmonary septum not aligned with interventricular septum and also have VSD Figure: Sadler 2004 Tetralogy of Fallot Combination of defects, seen in approx. 10 in 10,000births (0.10%). 1. Pulmonary stenosis 2. VSD 3. Overriding aorta 4. Hypertrophy of right ventricle Figure: Sadler 2004 Figure References • FitzGerald, M. J. T. (1977) Human Embryology: A Regional Approach. New York: Harper & Row Publ. • Gilbert, S. G. (1989) Pictorial Human Embryology. Seattle: Univ. Washington Press • Langebartel, D. A. & Ullrich, R. H. Jr. (1977) The Anatomical Primer: An Embryological Explanation of Human Gross Morphology. Baltimore: Univ. Park Press. • Larsen, W. J. (1993) Human Embryology. New York: Churchill Livingstone. • Moore, K. L. & Persaud, T. V. N. (1998) The Developing Human: Clinically Oriented Embryology. Philadelphia: W. B. Saunders Co. • Sadler, T. W. (2004) Langman’s Medical Embryology, 9th Ed. Philadelphia: Lippincott Williams & Wilkins.