Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
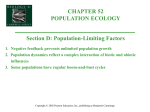
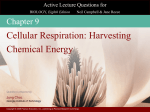
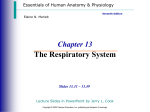
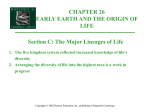
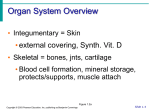
PowerPoint® Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Cardiovascular System 11 PART B Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings The Heart: Conduction System Intrinsic conduction system (nodal system) Heart muscle cells contract, without nerve impulses, in a regular, continuous way Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings The Heart: Conduction System Special tissue sets the pace Sinoatrial node = SA node (“pacemaker”), is in the right atrium Atrioventricular node = AV node, is at the junction of the atria and ventricles Atrioventricular bundle = AV bundle (bundle of His), is in the interventricular septum Bundle branches are in the interventricular septum Purkinje fibers spread within the ventricle wall muscles Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Heart Contractions Figure 11.6 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Heart Contractions Contraction is initiated by the sinoatrial node (SA node) About 75 beats per minute AV node can initiate pulse if needed, but at a much slower pace Force cardiac muscle depolarization in one direction—from atria to ventricles Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Heart Contractions Once SA node starts the heartbeat Impulse spreads to the AV node Impulse slows so atria can fill Then the atria contract At the AV node, the impulse passes through the AV bundle, bundle branches, and Purkinje fibers Blood is ejected from the ventricles to the aorta and pulmonary trunk as the ventricles contract Ventricles contract almost simultaneously Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Heart Contractions Figure 11.6 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Electrocardiography Used to make a visible record of the heart’s contractions Called an electorcardiogram EKG or ECG Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Electrocardiogram P Wave Depolarization of atria (contract) QRS Wave Repolarization of atria (rest) Depolarization of Ventricles T Wave Repolarization of Ventricles Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Figure 13.14 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Artificial Cardiac Pacemakers Continuously charging pacemakers Stimulate the heart at a set rhythm Demand Pacemakers Stimulate the heart only when it is below a set minimum Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Artificial Cardiac Pacemakers Inferior to the heart Can’t speed up the heart when necessary Can’t slow down when needed Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings The Heart: Regulation of Heart Rate Increased heart rate Sympathetic nervous system Crisis Low blood pressure Hormones Exercise Decreased blood volume Emotions Anxiety, fear, anger Increased blood temperature Epinephrine Thyroxine Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings The Heart: Regulation of Heart Rate Decreased heart rate Parasympathetic nervous system Cold receptors Emotions- grief and pain High blood pressure or blood volume Decreased venous return Release Acetylcholine (Ach) Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Cardiac Pressorflexes Receptors sensitive to changes in pressure (baroreceptors) Aortic baroreceptors Carotid baroreceptors Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Cardiac Pressorflexes Detect increase In blood pressure Sends to Brain Decrease in Blood Pressure Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings SA Node Releases Ach Heart Rate decreases Cardiac Arrythmia’s Arrythmia- abnormal beating of the heart Tachycardia—rapid heart rate over 100 beats per minute Bradycardia—slow heart rate less than 60 beats per minutes Sinus Arrythmias- variation of heart during breathing cycle Increases during inspiration Decreases during expiration Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings The Heart: Cardiac Cycle Complete heartbeat or pumping cycle Atria contract simultaneously Atria relax, then ventricles contract Systole = contraction Diastole = relaxation Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Filling Heart Chambers: Cardiac Cycle Left atrium Right atrium Left ventricle Right ventricle Ventricular filling Atrial contraction Mid-to-late diastole (ventricular filling) Isovolumetric Ventricular contraction phase ejection phase Isovolumetric relaxation Ventricular systole (atria in diastole) Early diastole Figure 11.7 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Filling Heart Chambers: Cardiac Cycle Left atrium Right atrium Left ventricle Right ventricle Ventricular filling Mid-to-late diastole (ventricular filling) Figure 11.7, step 1a Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Filling Heart Chambers: Cardiac Cycle Left atrium Right atrium Left ventricle Right ventricle Ventricular filling Atrial contraction Mid-to-late diastole (ventricular filling) Figure 11.7, step 1b Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Filling Heart Chambers: Cardiac Cycle Left atrium Right atrium Left ventricle Right ventricle Ventricular filling Atrial contraction Mid-to-late diastole (ventricular filling) Isovolumetric contraction phase Ventricular systole (atria in diastole) Figure 11.7, step 2a Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Filling Heart Chambers: Cardiac Cycle Left atrium Right atrium Left ventricle Right ventricle Ventricular filling Atrial contraction Mid-to-late diastole (ventricular filling) Isovolumetric Ventricular contraction phase ejection phase Ventricular systole (atria in diastole) Figure 11.7, step 2b Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Filling Heart Chambers: Cardiac Cycle Left atrium Right atrium Left ventricle Right ventricle Ventricular filling Atrial contraction Mid-to-late diastole (ventricular filling) Isovolumetric Ventricular contraction phase ejection phase Isovolumetric relaxation Ventricular systole (atria in diastole) Early diastole Figure 11.7, step 3 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Atrial Systole When atria contract Sends blood to ventricles AV valves are open SL valves closed Ventricles fill with blood Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Isovolumetric Ventricular Contraction (IVC) Before SL valves open Pressure in ventricle increases Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Ejection SL valves open Blood goes to ventricles Blood is ejected Residual Volume- the blood that remains in the heart at the end of the ejection period Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Isovolumetric Ventricular Relaxation (IVR) Between the closing SL valves and opening of AV valves AV valves won’t open until the pressure in the atrial chambers is above that in the relaxing ventricles Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Passive Ventricular Filling (PVR) When blood rushes into the ventricles and they fill up again Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Please note that due to differing operating systems, some animations will not appear until the presentation is viewed in Presentation Mode (Slide Show view). You may see blank slides in the “Normal” or “Slide Sorter” views. All animations will appear after viewing in Presentation Mode and playing each animation. Most animations will require the latest version of the Flash Player, which is available at http://get.adobe.com/flashplayer. Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Please note that due to differing operating systems, some animations will not appear until the presentation is viewed in Presentation Mode (Slide Show view). You may see blank slides in the “Normal” or “Slide Sorter” views. All animations will appear after viewing in Presentation Mode and playing each animation. Most animations will require the latest version of the Flash Player, which is available at http://get.adobe.com/flashplayer. Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Heart Sounds Heard through a stethoscope Lubb-dubb Systyolic sound First sound, longer and louder Caused by contraction of ventricle and closing of AV valves Diastolic sound Second sound, shorter and sharper Caused by closing of SL valves Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Hemodynamics Term to describe the changing circulation of blood Blood must be shifted from less active areas to more active areas Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Primary Principle of Circulation Control of circulation comes from Newton’s law of motion 1st law- fluid doesn’t flow when pressure is the same in all parts 2nd law- fluid only flows when pressure is higher in one area than in another Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Heart Sounds Heart murmur Incomplete closing of the valves Fairly common Most do not need treatment Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings The Heart: Cardiac Output Cardiac output (CO) Amount of blood pumped by each side (ventricle) of the heart in one minute Stroke volume (SV) Volume of blood pumped by each ventricle in one contraction (each heartbeat) Usually remains relatively constant About 70 mL of blood is pumped out of the left ventricle with each heartbeat Heart rate (HR) Typically 75 beats per minute Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Control of Arterial Blood Pressure Primary determinant of arterial blood pressure is volume of blood in arteries Arterial blood volume is directly proportional to arterial blood pressure Two most important factors influencing arterial pressure through their influence on arterial volume Cardiac output Peripheral resistance Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Cardiac Output Is the amount of blood pumped by each ventricle in one minute Primary indicator of the functional capacity of circulation to meet demands of physical activity Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Cardiac Output Stroke volume- volume of blood pumped by each ventricle in one contraction Heart rate is typically 75 beats per minute Q = S.V. x H.R. Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings The Heart: Cardiac Output CO = HR SV CO = HR (75 beats/min) SV (70 mL/beat) CO = 5250 mL/min The greater the stroke volume, the greater the cardiac output, but only if heart rate remains the same Anything that tends to change HR or SV tends to change Q, arterial volume, and arterial blood pressure in the same direction Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Target Heart Rate Maximum HR = 220-age Target HR = Max HR – resting HR x .7 + resting HR Any increase in cardiac output is directly proportional to an increase in action for aerobic metabolism Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Startling’s Law of the Heart The longer, or more stretched the heart fibers are at the beginning of a contraction, the stronger the contraction will be. Amount of blood in the heart determines how stretched the fibers are The more blood returned to the heart per minute, the more stretched the fibers are and the stronger the contraction is. Startling’s Law ensures that increase amounts of blood returned to the heart are pumped out of it Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Peripheral Resistance Peripheral resistance is the resistance to blood flow imposed by the force of friction between blood and the walls of its vessels Arterial blood pressure tends to vary directly with peripheral resistance Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Peripheral Resistance Causes of friction Viscosity- the thickness of blood Length of the vessel Diameter of the vessel Arterioles contract and dilate and change the resistance to blood flow. Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Peripheral Resistance Peripheral resistance determines pressure by controlling the rate of arteriole runoff The amount of blood that runs out of the arteries and into the arterioles The greater the resistance the less runoff and the more blood left in the arteries and the higher the blood pressure Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Peripheral Resistance Blood viscosity come from red blood cells The more red blood cells, the thicker the blood Anemia or hemorrhage can cause a decrease in blood viscosity, which can lower peripheral resistance and arterial blood pressure Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Vasomotor Control Mechanism Influence blood pressure by changing blood distribution (hemodynamics) and diameter of arterioles Smooth muscle of tunica media that allows this change Sympathetic fibers is smooth muscle of vessels cause them to constrict and increase pressure Dilate they decrease pressure Heat and alcohol causes vasodialation Nicotine, intense fear or anger, and cold causes vasocontriction and rise in blood pressure Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Vasomotor Pressorreflexes Cardiac baroreceptors Detect increase Pressure Decrease Heart Rate Inhibits Vasocontrictor center Pressure Decreases Vessel Dialates Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Vasomotor Pressorrelexes Located in the aorta and carotid artery Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Vasomotor Chemoreflexes Chemoreceptors located in the aortic arch and carotid body Sensitive to excess carbon dioxide- hypercapnia Less sensitive to deficiency of blood oxygenhypoxia Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Medullary Ischemic Reflex Activates when carbon dioxide builds up in the brain hypercapnia controls blood vessels to send oxygen to brain If too little oxygen, this system can’t operate Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Pulse Pulse Pressure wave of blood Monitored at “pressure points” in arteries where pulse is easily palpated Pulse averages 70–76 beats per minute at rest Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Venous Return to Heart Each time diaphram contracts, changes pressure in vena cava and causes blood to flow back to heart Skeletal muscle contractions act as booster pumps valves in veins prevent blood from falling back Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Minute Volume of Blood Minute Volume of blood amount of blood circulating through the body per minute Poiseuille’s Law Minute Volume = Pressure Gradient Peripheral Resistance Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Blood Pressure Measured with a sphygmomanometer amount of air pressure equal to arterial pressure Measured with the auscultatory method Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Measuring Arterial Blood Pressure Figure 11.20a Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Measuring Arterial Blood Pressure Figure 11.20b Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Measuring Arterial Blood Pressure Figure 11.20c Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Measuring Arterial Blood Pressure Figure 11.20d Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Systolic—pressure at the peak of ventricular contraction Diastolic—pressure when ventricles relax Write systolic pressure first and diastolic last (120/80 mm Hg) Pressure in blood vessels decreases as distance from the heart increases Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Comparison of Blood Pressures in Different Vessels Figure 11.19 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Blood Pressure: Effects of Factors BP is blood pressure BP is affected by age, weight, time of day, exercise, body position, emotional state CO is the amount of blood pumped out of the left ventricle per minute PR is peripheral resistance, or the amount of friction blood encounters as it flows through vessels Narrowing of blood vessels and increased blood volume increases PR BP = CO PR Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Blood Pressure: Effects of Factors Neural factors Autonomic nervous system adjustments (sympathetic division) Renal factors Regulation by altering blood volume When blood pressure too high, kidneys allow more water to leave body in urine, which results in thinner blood and decreased pressure Renin—hormonal control Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Blood Pressure: Effects of Factors Temperature Heat has a vasodilating effect Cold has a vasoconstricting effect Chemicals Various substances can cause increases or decreases Diet Debated, but some believe a diet low in salt, saturated fates and cholesterol will help prevent hypertension Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Variations in Blood Pressure Normal human range is variable Normal 140–110 mm Hg systolic 80–75 mm Hg diastolic Hypotension Low systolic (below 110 mm HG) Often associated with illness Hypertension High systolic (above 140 mm HG) Can be dangerous if it is chronic Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Arterial Vs. Venous Bleeding Blood escapes from an artery in spurts and gushes out Blood leaving a vein in a uniform fashion Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Velocity of Blood When a liquid flows from one cross-sectional size to an area with a larger cross-sectional size, its velocity slows Why would capillaries have a slow velocity? Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Pulse Mechanism The alternate expansion and recoil of an artery A pulse can be felt because arterial walls can expand and contract Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Where can pulse be felt Can be felt wherever an artery lies over a bone Common pulse points Radial artery Carotid artery Brachial artery Femoral artery Facial Artery Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Pulse Figure 11.18 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Pulse Wave Pulse wave dissipates as it travels away from the heart Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Venous Pulse Only exists in large veins Not as important as arterial pulse Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Exchange Substances exchanged due to concentration gradients Oxygen and nutrients leave the blood Carbon dioxide and other wastes leave the cells Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Exchange: Mechanisms Direct diffusion across plasma membranes Endocytosis or exocytosis Some capillaries have gaps (intercellular clefts) Plasma membrane not joined by tight junctions Fenestrations (pores) of some capillaries Found where absorption is a priority like intestinal capillaries Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Capillary Exchange: Mechanisms Figure 11.22 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Fluid Movements at Capillary Beds Blood pressure forces fluid and solutes out of capillaries Osmotic pressure draws fluid into capillaries Blood pressure is higher than osmotic pressure at the arterial end of the capillary bed Blood pressure is lower than osmotic pressure at the venous end of the capillary bed Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Fluid Movements at Capillary Beds Figure 11.23 Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Developmental Aspects of the Cardiovascular System A simple “tube heart” develops in the embryo and pumps by the fourth week The heart becomes a four-chambered organ by the end of seven weeks Few structural changes occur after the seventh week Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Congenital Heart Defects Congenital means present at birth Maternal infection and ingestion of drugs during first three months of pregnancy are major causes Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Aerobic Exercise and the heart Heart will hypertrophy and cardiac output increases if exercise regularly aerobically Pulse rate and blood pressure decrease Clears fatty deposits from blood vessel walls Must be regular exercise Many weekend athletes are myocardial infarction victims Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Developmental Aspects of the Cardiovascular System Aging problems associated with the cardiovascular system include Venous valves weaken Varicose veins Progressive atherosclerosis Loss of elasticity of vessels leads to hypertension Coronary artery disease results from vessels filled with fatty, calcified deposits Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Certified Surgical Technologist Use their knowledge of anatomy to assist surgeons Keep operating area sterile Use knowledge of surgical tools to assist physician Must anticipate Dr.’s next move and are their extra eyes during a procedure Must complete an accredited training program and pass national certifying exam Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Cycle of Life As a person ages, blood pressure increases As a person ages, pulse rate decreases Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Hypertension Cause of most office visits to physicians 140/90 is hypertension Primary Hypertension- has no known cause Secondary Hypertension Caused by pregnancy, kidney disease, or other cause Genetics play a huge role Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Hypertension Males have higher rates of hypertension Women more likely to die from a heart attack Tends to be higher in African Americans Direct relationship between age and hypertension Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Hypertension Other risk factors include Obesity Calcium deficiencies High alcohol and caffeine intake Smoking Lack of exercise Type “A” personalities Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Hypertension Complications of untreated hypertension Ischemic heart disease and heart failure Kidney failure stroke Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Hypertension Known as the “silent killer” No overt signs Headaches, dizziness, and fainting may occur Need regular screenings to detect Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Orthostatic Hypertension Temporary low blood pressure and dizziness when rising suddenly from a reclining position Common among elderly Aging sympathetic system reacts slowly to postural changes and blood pools in lower limbs Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Circulatory Shock Failure of the circulatory system to adequately deliver oxygen to the tissues Many types of circulatory shock Cardiogenic Shock Results from any type of heart failure Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Circulatory Shock Hypovolemic Shock Results from the loss of blood volume in the blood vessel which leads to low blood pressure Hemmorhage is a common cause Also caused by loss of interstitial fluid common in chronic diarrhea, vomiting, dehydration, or severe burns Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Circulatory Shock Neurogenic Shock Results from widespread dilation of blood vessels Caused by injury to the spinal cord or medulla, depressive drugs, Anaphylatic Shock Results from allergic reaction Causes blood vessels to dialate Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings Circulatory Shock Septic Shock Complication where infectious agents release toxins into the blood Copyright © 2009 Pearson Education, Inc., publishing as Benjamin Cummings