Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
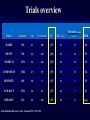
QUAND PROPOSER UN TRAITEMENT ELECTRIQUE ? Prof L DE ROY Université de Louvain CLINIQUES UNIVERSITAIRES UCL DE MONT-GODINNE Belgique J Am Coll Cardiol 2002;40:1703–19 Recommendations for ICD Therapy LVEF≤35% Class I (A) MADIT I P=0.009 Moss AJ, N Engl J Med 1996;335:1933-40 Class II a (B) Buxton AE,, N Engl J Med 1999 MUSTT LVEF≤30% MADIT II P=0.007 Moss AJ, N Engl J Med 2002;346:877-83 J Am Coll Cardiol 2002;40:1703–19 Pacing Recommendations for Dilated Cardiomiopathy P<0.001 MUSTIC P<0.001 J Am Coll Cardiol 2002;40:1703–19 MUSTIC MIRACLE N Engl J Med 2001;344:873-80 P=0.03 N Engl J Med 2002;346:1845-53 Swedberg et al., EHJ 2005;26:1115-1140 CRT Pacemakers Swedberg et al., EHJ 2005;26:1115-1140 CRTP -CRTD N Engl J Med 2004;350:2140-50 CRTP Class I B Cleland JG, N Engl J Med 2005;352:1539-1549 CARE-HF trial : extension phase Worsening heart failure All cause mortality Sudden cardiac death Cleland et al Eur Heart J 2006;27:1928-32 ICD – ICD +CRT ICD +CRT Class II a (B) (COMPANION) Class I (A) (AVID) ICD Class I (A) (MADIT II/SCD HeFT) Swedberg et al., EHJ 2005;26:1115-1140 Class II a (B) Hunt SA,Circulation 2005;20: e154-e685 Stage C Therapy:Reduced LVEF with Symptoms Cardiac Resynchronization (CRTP / CRTD) I IIa IIb III Hunt SA,Circulation 2005;20: e154-e685 CARE-HF The use of an ICD in combination with CRT should be based on the indications for ICD therapy. Stage D Therapy Inform on option to inactivate defibrillation I IIa IIb III Patients with refractory end-stage HF and implantable defibrillators should receive information about the option to inactivate defibrillation. Characteristics of patients enrolled and QRS eligibility criteria of the major RCTs on CRT Boriani G., J Interv Card Electrophysiol 2007 Results of cardiac resynchronization in CHF from CRT* *with estimated extent of effect Boriani G., J Interv Card Electrophysiol 2007, feb 24 Indication to CRT according to recent ACC/AHA guidelines CL I (A) Boriani G., J Interv Card Electrophysiol 2007 Qu’en est-il de l’asynchronisme et QRS fins Magnitude of Improvement in Clinical and Echocardiographic Parameters After CRT* n =33 n =33 Bleeker GB, J Am Coll Cardiol 2006;48:2243–50 Changes in LVESV, LVEDV, and EF in HF pts with narrow QRS complexes with/without significant systolic asynchrony according to asynchrony index Left ventricular end-systolic vol. Left ventricular end-diastolic vol. N=102 Left ventricular ejection fraction Yu CM.,J Am Coll Cardiol 2006;48:2251–7 Qu’en est-il de la classe IV Time to mode of death by treatment arm for NYHA class IV in COMPANION trial CRTD CRT N=217 A. Time to sudden death B. Time to HF death Lindenfeld JA, Circulation. 2007;115:204-212 FAUT-IL ADJOINDRE SYSTEMATIQUEMENT UN DAI A LA CRT ? Residual risk of sudden cardiac death in heart failure beta-blocker trials Field M, J Interv Card Electrophysiol, 2007 Survival for biventricular ICD and biventricular PM Ermis C, J Cardiovasc Electrophysiol 2004(15):862-866 CRTD VS CRT META-ANALYSIS OF COMPANION + ERMIS: ALL CAUSE MORTALITY: OR = 0.69 (0.53,0.91) P= 0.008 ABDULLA 2006 Estimated annualized sudden cardiac death rates in patients with nonischemic dilated cardiomyopathy receiving medical therapy Field M, J Interv Card Electrophysiol, 2007 7.5 RE-HF NNT Resynchronisation NNT HF studies NNT HF studies 30 25 NNT 20 15 26 10 5 11 14 17 14 11 17 20 20 14 7.5 0 MADIT COMPANION II MADIT CARE-HF II 1 an 3 ans CRT-D CRT-P COPERNICUS MADIT II 1 an Carvedilol MADIT SAVE II COPERNICUS MERIT-HF SAVE 3.5 ans Captopril 1 an Succinate de metoprolol Aurrichio et al, Circulation 2004, 109; 300 - 307 Number of patients with NYHA class IV heart failure enrolled in primary prevention ICD trials Field M, J Interv Card Electrophysiol, 2007 Percentage of patients after 2 years survival with sustained LV remodeling or an increase in absolute LVEF of 5% after CRT N=89 sustained LV remodeling means LV end systolic volume (LVESV) reduction of 10% Delnoy PP., J Cardiovasc Electrophysiol, 2007(18):298-302 NYHA class IV endpoints by treatment arm in COMPANION trial Secondary time to all-cause death N=217 Time to all-cause death or HF hospitalization Lindenfeld JA, Circulation. 2007;115:204-212 Primary time to all-cause death or hospitalization Death among patients with AF randomized to CRT vs RV pacing CRT: 49% reduction in the relative risk of all-cause mortality p=0.547 MUSTIC–AF: Multisite Stimulation in Cardiomyopathy Study–Atrial Fibrillation PAVE: Post AV Nodal Ablation Evaluation OPSITE: Optimal Pacing SITE Study Bradley DJ.,Heart Rhythm 2007;4:224 –232 Results of cardiac resynchronization in CHF from CRT* *with estimated extent of effect Boriani G., J Interv Card Electrophysiol, 2007 Effect of CRT on all-cause mortality Abdulla J.,Cardiology 2006;106:249–255 Identification des patients: les études en resynchronisation Patients MIRACLE NYHA III-IV FE< 35% QRS > 130 ms Φ LVED > 55mm Rythme sinusal CARE-HF COMPANION NYHA III-IV (+ de 6 sem) Ischémique ou non DTDS > 30 mm/m² FE <35% QRS > 120 ms Si 120 <QRS>149 ms 2 des critères suivants sont requis: • Retard pré-éjection Ao > 140 ms • Délai inter-vent mécan.> 40 ms • Retard activation postéro-lat. paroi vent. gauche NYHA III-IV CHF isch ou non Hospit dans l’année écoulée FE<35% Φ LVED > 60 mm QRS >120ms PR >150ms Rythme sinusal Rythme sinusal Devices CRT CRT - P CRT - D Bénéfices 1. Amélioration NYHA, périmètre de marche, QoL. 2. Réduit les hospitalisations pour IC et toutes causes 1. Réd. Mortalité tt causes - 36% 1. Réduction de la mortalité -36% 2. Réd. Hospitalisations - 52% 2. Réduc. Hospitalisations -37% 3. Amélioration des symptômes 4. Amélioration des capacités d’effort CARE-HF Critères d’inclusion : - NYHA III-IV, -QRS > 120ms, - LVEDD > 30 mm -FE < 35%. Objectifs primaires : - mortalité hospitalisation pour cause cardiovasculaire Pourcentage de mortalité - 40.0% 813 patients - 36% 30.0% p = 0.002 30.0% (82 centres en Europe) TMO TMO + CRT-P [404 patients] [409 patients] Etiologie HF Fraction d’éjection NYHA 1-2-3-4 [%] Durée du suivi Arythmies auriculaires Historique de diabète Durée du QRS QRS > 120 ms Test de marche 6 min 38% ischémique 26% 0 – 0 – 94 – 6 29.4 mois 21% 21% 165 ms 100% - ACE I Bétabloquant Diurétique Spironolactone Statine 80% 72% 99% 56% 39% 20.0% 20.0% 10.0% 0.0% Contrôle Thérapie CRT-P http://www.care-hf.com La réduction du risque absolu (RA) est de 9.4% (p = 0.002) après 29.4 mois. Elle (RA) grimpe à 13.4% (p<0.0001) après 36.4 mois (Care HF extension) Cleland JN Engl J Med. April 14, 2005;352:1539-1549 COMPANION Critères d’inclusion : -NYHA III-IV, -QRS > 120 ms, - PR interval > 150ms, -LVEDD > 60mm - EF < 35%. Objectifs primaires : mortalité ou hospitalisation Pourcentage de mortalité 40.0% 1.520 patients (128 centres au Etats-Unis) 30.0% - 36% TMO TMO + CRT-D TMO + CRT-P [308 patients] [595 patients] [617 patients] 20.0% 19.0% p = 0.003 12.0% Etiologie HF Fraction d’éjection NYHA 1-2-3-4 [%] Durée du suivi Arythmies auriculaires Historique de diabète Durée du QRS QRS > 120 ms Test de marche 6 min 59% ischémique 22% 0 – 0 – 86 – 14 12 mois 41% 160 ms 100% 258 m ACE I Bétabloquant Diurétique Spironolactone Statine 69% 68% 97% 55% - 10.0% 0.0% Contrôle Thérapie CRT-D Le défibrillateur associé à la resynchronisation diminue la mortalité de 36% (p = 0.003) par rapport au groupe contrôle. Bardy GH. N Engl J Med. January 20, 2005;352:225-237 Critères d’inclusion Remboursements AVID MADIT I Pt survivants de FV FV avec syncope FV avec FE < 40% + sympt ESC DAI Remboursements Mort subite Mort subite TV soutenue TV soutenue Pt NYHA I-III FE <35% Post infar asympt Tachy vent Patient IC symptomat. SCD- HeFT MADIT II CARE HF COMPANION Pt CHF FE<35% NYHA II-III DAI FE Basse < 30 – 35% Post MI > 40 j Pt NYHA I-III FE <30% Post infar asympt LVD Symptômes Syncope Périodes de vertige Bradycardie Prophylaxie HF Dysfonction cérébrale Pt NYHA III-IV FE <35 DTDS >30 mm/m QRS > 150 NYHA III-IV CHF isch ou non Hospit dans l’année écoulée FE<35% Φ LVED > 60 mm QRS >120ms PR >150ms Ethiologie Fibrose tissu de conduct. Post MI Congénital Chirurgical /complic. chir. Ablation Syndrome sinus carotid. Cardiomyop – Myocardite Maladie valvulaire NYHA III-IV CRT QRS Long > 120 ms FE altérée ECG CRT-D NYHA III IV FE Basse < 35% QRS Long > 120 ms AV Block Block Faisceau de Hiss Block de branche Syndrome sinusal Tachy atriale Tachy ventriculaire Life-Years Gained per Device Implanted Saluke TV,Circulation, 2004;109:1848-1853 Meta-analysis of trials comparing ICD with control on mortality in patients with heart failure and/or left ventricular systolic dysfunction Cleland JGF,The European Journal of Heart Failure 6 (2004) 501–508 All-cause mortality among patients with NICM randomised to ICD vs medical therapy in secondary prevention NICM=nonischemic cardiomyopathy Desai AS, JAMA 2004;292/2874-2879 Total annual costs of New York Heart Association class III–IV heart failure patients Field M, J Interv Card Electrophysiol, 2007 LV ejection fraction after CRT at 2 years survival P<0.001 Delnoy PP., J Cardiovasc Electrophysiol, 2007(18):298-302 Number of patients with NYHA class IV heart failure enrolled in primary prevention ICD trials Field M, J Interv Card Electrophysiol, 2007 Effect of ICD on cardiac death in randomized controlled trials Abdulla J.,Cardiology 2006;106:249–255 Patients With Cardiac Structural Abnormalities or Remodeling Who Have Not Developed HF Symptoms Class I 1. All Class I recommendations for Stage A should apply to patients with cardiac structural abnormalities who have not developed HF. (Levels of Evidence: A, B, and C as appropriate) 2. Beta-blockers and ACEIs should be used in all patients with a recent or remote history of MI regardless of EF or presence of HF. (Level of Evidence: A) 3. Beta-blockers are indicated in all patients without a history of MI who have a reduced LVEF with no HF symptoms (see Table 3 and text). (Level of Evidence: C) 4. Angiotensin converting enzyme inhibitors should be used in patients with a reduced EF and no symptoms of HF, even if they have not experienced MI. (Level of Evidence: A) Hunt SA,Circulation 2005;20: e154-e685 Patients With Cardiac Structural Abnormalities or Remodeling Who Have Not Developed HF Symptoms Class I 5. An ARB should be administered to post-MI patients without HF who are intolerant of ACEIs and have a low LVEF. (Level of Evidence: B) 6. Patients who have not developed HF symptoms should be treated according to contemporary guidelines after an acute MI. (Level of Evidence: C) 7. Coronary revascularization should be recommended in appropriate patients without symptoms of HF in accordance with contemporary guidelines (Level of Evidence: A) 8. Valve replacement or repair should be recommended for patients with hemodynamically significant valvular stenosis or regurgitation and no symptoms of HF in accordance with contemporary guidelines. (Level ofEvidence: B) Hunt SA,Circulation 2005;20: e154-e685 Patients With Cardiac Structural Abnormalities or Remodeling Who Have Not Developed HF Symptoms Class IIa Placement of an ICD is reasonable in patients with ischemic cardiomyopathy who are at least 40 days post-MI, have an LVEF of 30% or less, are NYHA functional class I on chronic optimal medical therapy, and have reasonable expectation of survival with a good functional status for more than 1 year. (Level of Evidence: B) Class IIb Placement of an ICD might be considered in patients without HF who have nonischemic cardiomyopathy and an LVEF less than or equal to 30% who are in NYHA functional class I with chronic optimal medical therapy and have a reasonable expectation of survival with good functional status for more than 1 year. (Level of Evidence: C) Hunt SA,Circulation 2005;20: e154-e685 Applying Classification of Recommendations and level of evidence Hunt SA,Circulation 2005;20: e154-e685 Major implantable ICD trials Zipes DP,Europace 2006(8):746-837 Swedberg et al., EHJ 2005;26:1115-1140 N Engl J Med 2004;350:2140-50 Zipes DP, Europace 2006(8):746-837 Ventricular arrhythmia and sudden cardiac death related to specific pathology Left ventricular dysfunction due to prior myocardial infarction Recommendations for ICD implantation Class I Zipes DP, Europace 2006(8):746-837 Placement of an ICD is reasonable in patients with ischemic cardiomyopathy who are at least 40 days post-MI, have an LVEF of 30% or less, are NYHA functional class I on chronic optimal medical therapy, and have reasonable expectation of survival with a good functional status for more than 1 year. Hunt SA,Circulation 2005;20: e154-e685 I IIa IIb III SCD-HeFT Bardy GH, N Engl J Med 2005;352:225-37 Patients With Current or Prior Symptoms of HF, With Reduced LVEF I IIa IIb III Hunt SA,Circulation 2005;20: e154-e685 SCD-HeFT Bardy GH, N Engl J Med 2005;352:225-37 Stage D Therapy Recommended Therapies Include: •Control of fluid retention •Referral to a HF program for appropriate pts •Discussion of options for end-of-life care •Informing re: option to inactivate defibrillator •Device use in appropriate patients •Surgical therapy – •Cardiac transplantation •Mitral valve repair or replacement •Other •Drug Therapy – •Positive inotrope infusion as palliation in appropriate patients (MADIT II (MADIT II Swedberg et al., EHJ 2005;26:1115-1140 P<0.02 AVID N Engl J Med 1997;337:1576-83 LES RECOMMENDATIONS Stage B Therapy:Asymptomatic LV dysfunction ICD I IIa IIb III I IIa IIb III Placement of an ICD is reasonable in patients with ischemic cardiomyopathy who are at least 40 days post-MI, have an LVEF of 30% or less, are NYHA functional class I on chronic optimal medical therapy, and have reasonable expectation of survival with a good functional status for more than 1 year. (MADIT II) Placement of an ICD might be considered in patients without HF who have nonischemic cardiomyopathy and an LVEF less than or equal to 30% who are in NYHA functional class I with chronic optimal medical therapy and have a reasonable expectation of survival with good functional status for more than 1 year. (DEFINITE, SCD-HeFT) Hunt SA,Circulation 2005;20: e154-e685 All-cause mortality among patients with NICM randomised to ICD or CRT-D vs medical therapy in primary prevention P=0.02 NICM=nonischemic cardiomyopathy Desai AS, JAMA 2004;292/2874-2879 Placement of an ICD might be considered in patients without HF who have nonischemic cardiomyopathy and an LVEF less than or equal to 30% who are in NYHA functional class I with chronic optimal medical therapy and have a reasonable expectation of survival with good functional status for more than 1 year. Hunt SA,Circulation 2005;20: e154-e685 SCD-HeFT I IIa IIb III Bardy GH, N Engl J Med 2005;352:225-37 Stages of Heart Failure At Risk for Heart Failure: STAGE A High risk for developing HF STAGE B Asymptomatic LV dysfunction Heart Failure: STAGE C Past or current symptoms of HF STAGE D End-stage HF Stage C Therapy:Reduced LVEF with Symptoms Recommended Therapies: •General measures as advised for Stages A and B •Drug therapy for all patients •Diuretics for fluid retention •ACEI •Beta-blockers •Drug therapy for selected patients •Aldosterone Antagonists •ARBs •Digitalis •Hydralazine/nitrates •ICDs in appropriate patients •Cardiac resynchronization in appropriate patients •Exercise Testing and Training Stage C Therapy:Reduced LVEF with Symptoms ICD I IIa IIb III I IIa IIb III An ICD is recommended as secondary prevention to prolong survival in patients with current or prior symptoms of HF and reduced LVEF who have a history of cardiac arrest, ventricular fibrillation, or hemodynamically destabilizing ventricular tachycardia. (AVID) ICD therapy is recommended for primary prevention to reduce total mortality by a reduction in sudden cardiac death in patients with ischemic heart disease who are at least 40 days post-MI, have an LVEF less than or equal to 30%, with NYHA functional class II or III symptoms while undergoing chronic optimal medical therapy, and have reasonable expectation of survival with a good functional status for more than 1 year. (MADIT II) Hunt SA,Circulation 2005;20: e154-e685 Patients With Current or Prior Symptoms of HF, With Reduced LVEF I IIa IIb III Hunt SA,Circulation 2005;20: e154-e685 P<0.02 N Engl J Med 1997;337:1576-83 Stage C Therapy:Reduced LVEF with Symptoms ICD I IIa IIb III ICD therapy is recommended for primary prevention to reduce total mortality by a reduction in sudden cardiac death in patients with nonischemic cardiomyopathy who have an LVEF less than or equal to 30%, with NYHA functional class II or III symptoms while undergoing chronic optimal medical therapy, and who have reasonable expectation of survival with a good functional status for more than 1 year. (DEFINITE; SCD-HeFT) I IIa IIb III Placement of an ICD is reasonable in patients with LVEF of 30% to 35% of any origin with NYHA functional class II or III symptoms who are taking chronic optimal medical therapy and who have reasonable expectation of survival with good functional status of more than 1 year. Hunt SA,Circulation 2005;20: e154-e685 Patients With Current or Prior Symptoms of HF, With Reduced LVEF I IIa IIb III Hunt SA,Circulation 2005;20: e154-e685 SCD-HeFT Bardy GH, N Engl J Med 2005;352:225-37 Patients With Current or Prior Symptoms of HF, With Reduced LVEF I IIa IIb III Hunt SA,Circulation 2005;20: e154-e685 MADIT II SCD-HeFT Bardy GH, N Engl J Med 2005;352:225-37 Moss AJ, N Engl J Med 2002;346:877-883 SCD-HeFT Trials overview Mortalité groupe Etudes # patients Age Coronariens FE Suivi (mois) MADIT 196 63 100 ≤ 35 27 17 54 MUSTT 704 66 100 ≤ 40 39 14 51 MADIT II 1232 64 100 ≤ 30 20 19 31 COMPANION 1520 67 59 ≤ 35 15 19 36 DEFINITE 458 58 0 ≤ 35 29 7 35 SCD-HeFT 2521 60 52 ≤ 35 46 7 23 DINAMIT 674 62 100 ≤ 35 30 8 neg Arch maladies du coeur et des vaisseaux 99, 2 141-154 contrôle RRR NNT Défibrillateurs NNT HF studies NNT 0 30 30 5 25 25 0 20 20 5 15 15 0 5 0 26 10 10 14 14 5 7.5 5 0 COMPANION SCD-HeFT CARE-HF 3.3 ans DAI 17 11 20 14 MADIT II MADIT II COPERNICUS 1 ans 2 ans 1 an 3.5 ans DAI DAI Carvedilol Captopril Aurrichio et al, Circulation 2004, 109; 300 - 307 SAVE MERIT-HF 1 an Succinate de metoprolol Le NNT des def. diminue avec le temps 133 133 140 123 120 100 1 an 80 2 ans 60 3 ans 40 24 21 20 11 3.3 1.7 8 4.6 11 17 8 11 15 5.6 4.7 2.5 0 MADIT AVID CIDS MADIT II CASH MUSTT Lifeyears gained from ICD implantation Saluke TV,Circulation, 2004;109:1848-1853 Brugada syndrome Recommendations for ICD implantation Class I Class IIa Class IIa Zipes DP, Europace 2006(8):746-837 Long QT syndrome Recommendations for ICD implantation Class I Class IIa Class IIb Zipes DP, Europace 2006(8):746-837 The CRT trials Behan MW,Int J Clin Pract, 2006, 60, 9, 1107–1114 Indications majeures de Défibrillateurs Classe Arrêt cardiaque • • • I A I B I B I B IIa B I B I B IIa B IIa B sur cardiopathie symptomatique TV soutenue spontanée II • • • mal tolérée TR ou ablation ayant échoué sans anomalie cardiaque Syncope • • • sans cause connue avec TV soutenue ou FV déclenchable avec anomalie cardiaque Patient avec maladie génétique • • à haut risque de mort subite par FV sans TRx connu Coronariens I • • • 1 mois après IM et 3 mois après revascularisation FE ≤ 35% arythmie ventriculaire déclenchable Coronariens II • Cardiopathies VF ou TV sans causes aiguë ou réversible TV soutenue spontanée I Trouble du rythme ventriculaire documenté Preuve Remboursement • • 1 mois post IM et 3 mois après revascularisation FE≤30% NYHA II ou III Insuffisance cardiaque • • • • NYHA III ou IV FE ≤ 35% QRS ≥ 120 ms TMO Cardiomyopathie dilatée • FE ≤ 35% Class III J Am Coll Cardiol 2002;40:1703–19 HOSPITALISATION Symptoms Class I A Class I A J Am Coll Cardiol 2002;40:111– 8 MIRACLE Class I A N Engl J Med 2002;346:1845-53 MADIT II P=0.007 Moss AJ, N Engl J Med 2002;346:877-883 Class I (A) MADIT II Swedberg et al., EHJ 2005;26:1115-1140 DEFINITE Moss AJ, N Engl J Med 2002;346:877-883 SCD-HeFT Kadish A, N Engl J Med 2004;350:2151-2158 Bardy GH, N Engl J Med 2005;352:225-237 SCD-HeFT trial DEFINITE DEFINITE P=0.006 Kadish A, N Engl J Med 2004;350:2151-2158 Bardy GH, N Engl J Med 2005;352:225-37