Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Quantium Medical Cardiac Output wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
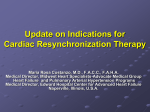
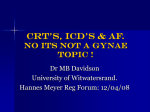
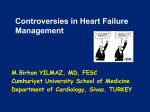
Heart Failure in 2012 Patricia P. Chang, MD MHS FACC Associate Professor, Medicine Director, Heart Failure & Transplant Program February 25, 2012 Disclosures • No relationships to disclose • I will discuss products that are investigational or used off-label Case • 55 yo BW presented to PCP with palpitations, ECG “abnormal” – Stress thallium (2003): no ischemia, LVEF 20%. – Exercises on treadmill 2 miles, 33 minutes, 3-4 d/week. No SOB, cp. Frequently naps during the day. Exam unremarkable except BMI 33. – PMH: carpal tunnel syndrome. No HTN, DM, h/o diet-controlled hyperlipidemia – FH: Father died MI age 67. No other CVD/HF/SCD • Presents to HF Clinic for further E/M • ACC/AHA Stage B, NYHA Class I • Further w/u? Treatment? Prognosis? Topics • • • • Epidemiology Evaluation: etiology, testing Common comorbidities Therapies and timing Disclaimer: More focus on Systolic HF vs HF with preserved EF Topics • • • • Epidemiology Evaluation: etiology, testing Common comorbidities Therapies and timing HF Estimates • HF affects 5.7 Million: 3.1 M men, 2.6 M women (self-report, age ≥20yo, NHANES-2008) • Lifetime risk 20% (≥40yo, Framingham[FHS]) • Hospitalizations > 1 M / year • Prevalence and Incidence of HF increases with age – 670,000 new cases age ≥45yo (FHS) – 56,000 deaths; 1 in 9 deaths (NCHS) • ≥50% diagnosed w/ HF die within 5 yrs (Olmsted) Roger V et al. Heart Disease and Stroke Statistics—2011 Update. Circulation 2011;123(4):e18-e209. “Diastolic” vs Systolic HF Aurigemma GP, Gaasch WH. NEJM 2004;351:1097-105. Systolic HF vs HFpEF 4596 HF patients, Mayo Clinic Owan TE et al, NEJM 2006; 355(3):254 Survival by HF type Owan TE et al, NEJM 2006; 355(3):254 Survival by Gender • Olmstead County: N=4537 HF patients (1979-2000) by ICD-9-CM codes (98% (+) Framingham criteria) MEN Rogers VL et al, JAMA 2004;292:344 WOMEN Survival by Race & Gender Study Loehr L, Rosamond W, Chang PP, et al. Am J Cardiol 2008;101(7):1016-1022 SHF Survival by Etiology & Gender 5 RCTs (N=11642 [2851 F]): PRAISE, PRAISE-2, MERIT-HF, VEST, PROMISE Etiology may be more important Nonischemic Ischemic Frazier CG et al, JACC 2007;49(13):1450-8. Topics • • • • Epidemiology Evaluation: etiology, testing Common comorbidities Therapies and timing Practice Guidelines • ACC/AHA: 1995, 2001, 2005, 2009 my.americanheart.org Heart Failure: Stage vs Class Hunt SA et al. ACC/AHA Guidelines 2005 & 2001; Circulation 2001;104:2996. Farrell MH, Foody JM, Krumholz HM. JAMA 2002;287:890 Practice Guidelines • HFSA: 1999, 2006, 2010 www.hfsa.org • ESC: 2001, 2005, 2008 (2010) Etiology of Systolic HF • Coronary artery disease 2/3 (“ischemic cardiomyopathy”) • Hypertension (“hypertensive cardiomyopathy”) • Valvular disease (“valvular CM”) • Infectious (e.g., viral myocarditis, Chagas) • Cardiotoxins (e.g., alcohol, chemotherapy) • Infiltrative (e.g., amyloidosis, sarcoidosis, hemochromatosis, Wilson’s) • Peripartum CM • Stress-induced CM • Genetic (Familial) • Idiopathic (Dilated) CM Evaluation of New HF (after a good H&P) • Cardiac function/structure – ECHO (Cardiac MRI, MUGA) • Etiology – R/O CAD: cath vs stress vs CT – Serologies: TSH, ANA, Ferritin, HIV, SPEP/UPEP – Cardiac MRI – Family Hx: Genetic testing? Genomic Locations of Genetic Variants Associated with the Risk of MI and HF O'Donnell CJ, Nabel EG. N Engl J Med 2011;365:2098-2109 Representative Genomewide Association Studies (GWAS) of Common CVDs O'Donnell CJ, Nabel EG. N Engl J Med 2011;365:2098-2109 Familial DCM • New Idiopathic DCM dx = Familial in 20-35% (when 1st degree family members screened) • Point mutations in 31 autosomal and 2 Xlinked genes – But only account only for 30-35% genetic causes Hershberger RE, Siegfried JD, JACC 2011;57(16):1641-9 Genetic Testing • Genetics Clinic at UNC (Meadowmont) • Familion “send out” (www.familion.com) Topics • • • • Epidemiology Evaluation: etiology, testing Common comorbidities Therapies and timing Comorbidities • Affect sxs, Rx, prognosis • Cardiovascular – CHD & CHD risk factors: HTN, DM, metabolic syndrome, obesity – Valvular disease – Arrhythmias – Other atherosclerotic disease: PAD, stroke • Noncardiac comorbidities – Too many to list… but will highlight: • Anemia • Sleep apnea Anemia • ~25% in HF population – Etiology: hemodilution, Fe or Epo deficiency, CKD • 1-g/dL Hgb reduction associated with a 20% increase in risk of death Tang WH et al, JACC 2008;51:569-576; Anand I et al, Circulation 2004;110:149-154 • Treatment is relatively easy – Iron supplementation – IV iron (short-term) – Erythropoiesis-stimulating agents (short term) Obstructive Sleep Apnea (OSA) • Similar sxs as HF • Common (12-53%) but under-diagnosed • Thus undertreated Mild to No OSA Untreated OSA Wang H et al, JACC 2007;49(15):1625-31. Kasai T, Bradley TD, JACC 2011;57(2):119-27 [REVIEW] Topics • • • • Epidemiology Evaluation: etiology, testing Common comorbidities Therapies and timing Standard HF Therapy • Guidelines (Systolic HF > HFpEF) – ACC/AHA: 1995, 2001, 2005, 2009 – HFSA: 1999, 2006, 2010 • Medications – Diuretics, ACE inhibitors* &/or Angiotensin receptor blockers* &/ or Hydralazine/Nitrates*, Beta-blockers*, Aldosterone antagonists*, Digoxin • Electrophysiology (EP) Devices – Implantable cardioverter defibrillator (ICD) – Biventricular pacemaker (CRT) • Surgery – – – – – Revascularization Ventricular restoration (Dor procedure) Mitral valve surgery Cardiac transplantation Mechanical circulatory support (VAD) HF Stages and Therapies Stem cells? Hemofiltration? ARB, H/I in some. ICD all Jessup M, Brozena S. NEJM 2003;348:2007 Stepwise Therapy for HF , B-blockers Kittleson MM, Kobashigawa JA, Circulation 2011;123:1569-1574 HF Specific Management • Identify and avoid exacerbating factors for HF • Behavioral management – – – – – – Fluid restriction (2 L = ½ gallon) Salt restriction (2 g) Daily weights (?sliding scale diuretics for the savvy) Exercise a.k.a. HF Core Measures Medical adherence No smoking • Biomarkers: BNP/NT-proBNP – New ones but not commonly available (ST2, endoglin, galectin3, cystatin C, neutrophil gelatinase-associated lipocalin, midregional proadrenomedullin, chromogranin A, adiponectin, resistin, leptin) • “Baseline/dry” weights & NTproBNP helpful Timing: Medications • Begin with ACC/AHA Stage A • Optimize for Stages B-D Timing: Medications • Lots of meds with good data, but challenges of polypharmacy – Compliance, cost, HF severity • Priorities – B-blocker, ACE-I for all (aim for target doses) – ARB as ACE-I alternative or if congested/ hypertensive – Hydralazine/nitrate if African-American or congested/hypertensive – Diuretic PRN and/or Aldosterone blocker – Digoxin if recurrent hospitalization Aim for Target Doses ACE-I BB Enalapril (Vasotec) Captopril (Capoten) Ramipril (Altace) Lisinopril (Prinivil, Zestril) Trandolapril (Mavik) Quinapril (Accupril) Bisoprolol (Zebeta) Carvedilol (Coreg) Metoprolol XL/CR (Toprol XL) Metoprolol (Lopressor) Atenolol (Tenormin) 10 mg bid 50 mg tid* 5 mg bid 20 mg qd 4 mg qd 20-40 mg bid § 10 mg qd 25-50 mg bid ** 200 mg qd 100 mg bid § ‡ 100 mg qd § ‡ *affected by food, ** depends on weight § no mortality data, ‡ not in guideline Hospitalized Pt: ADHF • IV diuretics – Bolus or continuous • IV vasodilators – Nitroglycerin, Nesiritide, Nitroprusside • IV inotropes Advanced, – Milrinone, Dobutamine, Dopamine End-stage • Optimize PO regimen Systolic HF Hunt SA, et al. ACC/AHA HF Guidelines Update. Circulation 2009;119(14):e391-479. Alternatives to Drugs • Ultrafiltration (aquapheresis therapy): – Peripheral or central venous access, ≤4 L off in ≤8 hrs, max removal rate 500 mL/hour – UNLOAD trial: n=200, RCT, UF vs IV diuretics • At 48 hrs, UF group had 38% weight loss, 28% net fluid loss • At 90 days after hospital d/c, UF had HF rehospitalizations, ED or clinic visits Costanzo MR et al. JACC 2007;49(6):675-83 • EECP (enhanced external counterpulsation) – Already used for angina pts – PEECH trial: n=187, RCT, EECP vs usual care • EECP pts had exercise time, QOL, NYHA Class, but no difference in peak VO2 changes Feldman AM et al. JACC 2006;48(6):1198-205 Implantable Cardioverter Defibrillator LVEF ≤35% • 2° Prevention – AVID (1997) • 1° Prevention – – – – MADIT (1996) MUSTT (1999) (EF 35-40%, +EPS) MADIT II (2002) SCD-HeFT (2004) ACC/AHA/ESC guidelines • Class I: LVEF ≤ 35%, NYHA II-III, ICM LVEF ≤ 30%, NYHA I • Class II: NICM LVEF ≤ 30% NYHA I Timing: ICD • • • • 40+ days post-MI/revascularization >3 months for NICM on optimal therapy Life expectancy >1 year Still, low referral rate – 42% (LVEF≤35%) & 49% (LVEF≤30%) eligible pts were referred (1 center, 2002-2006) Bradfield J et al, PACE 2009; 32:S194–S197 – Why? NNT = 6 (MADIT-II) to 14 (SCD-HeFT) • Patient vs Doctor? ICD implant rates overall low MADIT II eligible pts in GWTG hospitals –Implanted or Planned Implant rate: 20% overall <1% lowest tertile 35% highest tertile Shah B et al, JACC 2009;53(5):416-22 ICD Implant Rates Highest in large centers with sophisticated cardiac facilities Shah B et al JACC 2009;53(5):416-22 Reiterate the Message? • Life-saving • Prognostically Important ICD Shocks = Poor Prognosis Any shock is bad More shocks are worse • 33% SCD-HeFT pts received ≥1 ICD shock (128 pts appropriate, 87 inappropriate, 54 both types) • Most common cause of death = progressive HF Poole JE et al, NEJM 2008;359:1009-17 ICD Shocks = Poor Prognosis Cardiac Resynchronization Therapy • 30% with chronic HF have Ventricular Dyssynchrony • CRT with biventricular pacemakers can improve symptoms & survival*: NYHA Class III-IV, LVEF <35%, basal QRS duration of >120 msec – MUSTIC (QRS >150 ms) (2001) – MIRACLE (QRS >130 ms) (2002) – COMPANION (QRS >120 ms) (2004) – CARE-HF (QRS >120 ms) (2005)* Timing: CRT • After medical therapy optimized • CRT has been mostly studied in the NYHA III-IV population – If CRT, HF = “Advanced” • Consider CRT earlier? (earlier than NYHA Class III) – REVERSE Trial (2008) – MADIT-CRT Trial (2009) – RAFT Trial (2010) REVERSE Trial • 610 pts NYHA Class I-II, QRS ≥120, LVEF ≤40%: CRT-ON ▲ vs CRT-OFF ● Linde C et al, JACC 2008;52:1834-43 REVERSE Trial • ~96% on ACEi/ARB and BB; ~35% at target BB dose • ~80% NYHA II Linde C et al., JACC 2008;52:1834-43 MADIT-CRT • 1820 pts NYHA I-II, QRS≥130, LVEF≤30%: CRT-ICD vs ICD • ~40% NYHA II; 10% NYHA III-IV prior to enrollment Moss AJ et al, N Engl J Med 2009;361:1329-38. RAFT • 1789 pts, NYHA II-III, LVEF ≤30, QRS ≥120 or ≥200 paced: CRT-ICD or ICD Tang AS et al, N Engl J Med 2010;363:2385-95. CRT “Subgroups” • Pts who seem to benefit more: – QRS >150 msec (MADIT-CRT, RAFT) – Women (MADIT-CRT) Reverse Remodeling MADIT-CRT Moss AJ et al, N Engl J Med 2009;361:1329-38. • Responders: LA volume <40 ml/m2, women, nonischemic CM, LBBB, QRS ≥150, LVEDV ≥125 ml/m2, prior hospitalization for HF Goldenberg I et al, Circulation 2011;124(14):1527-36 CRT Limitations • ~30% do not respond to CRT JACC 2009;53:1933-1943) • HF does ultimately progress (PROSPECT, Bax JJ et al, Patient Preferences • Time trade (survival time vs perfect health) • Baseline: median trade for better quality = 3 months' survival time • Preferences in favor of survival for many pts despite advanced HF sxs, stable over time, but increase after hospitalization in 68% Stevenson LW et al, JACC 2008;52:1702-8 Heart Transplantation • The only “cure” • >89,000 Heart Tx worldwide, >50,000 in US (1988-) Hunt SA, Haddad F, JACC 2008:52:587-98. Hunt SA. NEJM 2006;355:3 Transplant Eligibility J Heart Lung Transplant 2006;25:1024–42. • Objective assessment of functional capacity (limitation) – 6 minute walk – Cardiopulmonary exercise stress test (CPX) • Peak exercise O2 consumption (VO2) The Problem: Organ Shortage • 4,000 pts are listed annually • Yearly wait list mortality 10% Gridelli and Remuzzi, NEJM 2000;303:404. Mechanical Circulatory Support: Ventricular Assist Devices: Bridge to Tx, Destination Therapy • Volume Displacement – – – – Thoratec Novacor Heartmate LVAS Abiomed • Axial Flow – Heartmate II – Jarvik • Centrifugal – CentriMag – Heartware Baughman KL, Jarcho JA. NEJM 2007;379(9):846-9. Timing: Transplant / VAD • • • • On optimal therapy (meds, EP devices) Progressive “advanced” HF (NYHA III-IV) Before truly “end stage” Failure of maximal medical therapy – Progressive HF symptoms – More arrhythmias • Evaluation is multidisciplinary, similar to transplant • Goal: ↑ quality and quantity of life Real Patients Timing: Transplant / VAD • Clinical Risk Factors for 1-yr Mortality Russell SD, Miller LW, Pagani FD, CHF 2008;14(6):316-21 – – – – – – – Walk <1 block without dyspnea Na <136 mEq ⁄ L BUN >40 mg ⁄dL or creatinine >1.8 mg ⁄dL Can’t tolerate ACEI ⁄ ARB ⁄ BB Diuretic dose >1.5 mg ⁄ kg ⁄ d HF admission in past 6 months No clinical improvement with CRT therapy, or no CRT and QRS >140 ms – Hematocrit <35% • Multiple risk models Heart Failure Survival Score For 1-year event-free survival Aaronson KD et al, Circulation 1997;95(12):2660-7 Reference for Table: Mehra MR et al, J Heart Lung Transplant. 2006:1024-42. This pt’s abs value sum score = 7.28 Seattle Heart Failure Model Levy WC et al. Circulation 2006;113:1424-1433 www.SeattleHeartFailureModel.org Systolic HF: Multidisplinary Care • Primary Care Provider • General Cardiologist • Heart Failure Cardiologist • Cardiac Surgeon • EP Cardiologist Summary • • • • • Systolic HF is common Always R/O CAD Do thorough FH R/O and Rx sleep apnea and anemia Aim for target doses for evidencebased HF pharmacologic therapies Stepwise Therapy for SHF Start Rx for ACC/AHA Stage A Optimize Rx for Stages B-D as follows: , behavioral modifications , B-blockers Stage B Stage C Kittleson MM, Kobashigawa JA, Circulation 2011;123:1569-1574 Stage D Summary • Aim for target doses for evidence-based HF pharmacologic therapies • ICDs underutilized, yet prognostically important • CRT can be considered earlier than “advanced stage”, but certain subgroups respond better • If still symptomatic beyond optimal behavior, meds, and EP devices, consider HTx and VAD – Always better to consider these therapies early vs too late UNC Heart Failure Team www.uncheartandvascular.org Cardiology (ph 919-843-5214) Cardiothoracic Surgery Pager 919-123-HEART (123-4327) (ph 919-966-3381) Brett Sheridan, MD Patricia Chang, MD MHS [email protected] [email protected] Andy Kiser, MD Brian Jensen, MD [email protected] [email protected] Tracy Vernon-Platt, ANP Carla Sueta, MD PhD [email protected] [email protected] Michael Mill, MD Kirkwood Adams Jr, MD Jana Glotzer, ACNP [email protected] [email protected] Transplant Coordinators (ph 919-966-4728) Scott Kowalczyk, RN BSN CCTC [email protected] Katie McMahon, RN BSN Jason Katz, MD MHS [email protected] [email protected] VAD Coordinators (pgr 919-216-2095) Mandy Bowen, RN BSN [email protected] Heart Failure NP Sarah Waters, ANP [email protected] Danielle Miller, RN BSN [email protected] 1-866-862-4327 = 866-UNC-HEART UNC Center for Heart and Vascular Care One Call Referral Service