Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
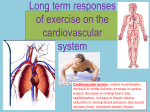
Cardiac Adaptation to Exercise chronic Morphological Functional •Myocardial •Neural •Vascular Chronic Cardiac Adaptation to Exercise Morphological Myocardial hypertrophy Coronaries CRMS Chronic Cardiac Adaptation to Exercise Morphological Myocardial hypertrophy •Eccentric •Concentric Coronaries CRMS Hypertrophia-Hyperplasia • Hyperplasia constitutes an increase in the number of cells in an organ or tissue, which may then have increased volume. • Hypertrophy refers to an increase in the size of cells and, with such change, an increase in the size of the organ Myocardial hypertrophy pressure overload Due to physical stimuli volume overload Due to hormonal chemical stimuli CRMS Factors promoting Cardiac hypertrophy Mechanical Force CRMS Development of Myocardial Hypertrophy Pressure Overload Volume Overload Increased parietal systolic stress Increased parietal diastolic stress Addition of sarcomer in parallel Addition of sarcomer in series Increase wall thickness Increase chamber size Concentric Hypertrophy Collagen Eccentric Hypertrophy CRMS Effects of pressure/volume overload on cardiac structure and function Exercise (Isometric-Isotonic) Overload Volume/pressure Adeguate Capillary density Myocite Hypertrophy Cardiac remodelling Increase contrattility Athletic Heart CRMS Effects of Training on Left Ventricle Adaptation of the Heart to Exercise Training Adaptation of the Heart to Exercise Normal Concentric Eccentric Calculation of Left Ventricle Mass LVM(gr) =0,80x1,05x (IVS+PWT+LVID)3-LVID CRMS 3 Anatomical Section Through the Short Axis of Left Ventricle Short Axis View of Left Ventricle in Normal Subject Short Axis View of Left Ventricle in Athlete Pathological Hypertrophy Hypertrophy Modulating Factors 1. Age 2. Gender 3. Type of stimulus 4. Genetic heritage CRMS Hypertrophy Modulating Factors • Age Left Ventricular Mass in young athletes ( soccer players): a cross echocardiographic study Giorgio Galanti M.D, Paolo Manetti M.D., Maria Concetta Vono M.D., Loira Toncelli M.D., Paola Zilli M.D., Carlo Rostagno M.D., Vieri Boddi M.Sc.*, Natale Villari M.D**,Roberto Salti M.D. CRMS • Purpose - Regular exercising induces changes in left ventricular mass (LVM). While its effects in adults are well known, few data are so far available on those in adolescents. • Methods - group of 127 young male soccer players (aged 13.6±2.1 yr., mean ± standard deviation) was studied. They had been regularly playing soccer since they were six years old. Players were age-matched with 70 male sedentary adolescents. LVM was detected with echocardiography and body composition with bioelectrical impedance analysis. Pubertal stadiation was evaluated with the Tanner method and skeletal maturation with hand x-ray. Results - Skeletal age, Tanner maturation and weight were comparable in the two groups, while height (p=0.002), fat-free mass (FFM, p<0.0005) and cellular body mass (p=0.002) were higher in athletes. Players showed increased LVM as compared with controls (159±49 vs. 137±42 g, p=0.002; confirmed by measures of LVM/body surface area: 97±19 g/m2 vs. 87±17 g/m2, p<0.0005, respectively). Starting from similar values, LVM progressively increased more in players than in controls after 12 yr. (Tanner 2), reaching statistical significance at 15.4 yr. (Tanner 5). In both athletes and controls LVM was directly correlated with all the anthropometric and cardiovascular parameters examined (p<0.0005). At multivariate analysis LVM was significantly correlated with skeletal age (b=8.54), height (b=1.77) in athletes, and with skeletal age (b=4.83) and FFM (b=1.83) in controls. Conclusions • Our data suggest that exercise induces a physiological left ventricular hypertrophy in sportive population. • This hypertrophy becomes evident after sexual maturation was achieved. Hypertrophy Modulating Factors Type of stimulus CRMS Hypertrophy Modulating Factors Circulation Reasearch 2001 Hypertrophy Modulating Factors Genetic Heritage Studied Subjets Allelic Frequency Analysis •42 elite soccer male players (from 17 to 31 years old) •45 age matched healthy male controls All were studied with echocardiography and DNA analysis G.Galanti et al. MSSE Nov:2000 Correlation between Left Ventricular Mass (LVM) and I/D Polimorphysm Genotype DD + ID II Athletes with increased LVM Athletes without increased LVM 14 5 0 3 p<0,05 G.Galanti et al. MSSE Nov:2000 CONCLUSIONS • Increase of left ventricular mass is correlated with I/D polimorphism: The DD athletes had shown an increase while the II athletes had a reduction. • Increase of left ventricular mass is not correlated with A/C polimorphism: CRMS G.Galanti et al. MSSE Nov:2000 La scelta dello sport è geneticamente determinata? Association of angiotensin-converting enzyme gene I/D polymorphism with change in left ventricular mass in response to physical training Montgomery H, Clarkson P et al Circulation 1997, 96: 741-747) CRMS Soggetti Studiati I soggetti studiati comprendevano 136 atleti allenati (età media 24±3.5 anni) tra i quali 121 erano calciatori (85 maschi, 36 femmine) e 15 ciclisti (maschi), confrontati con 155 controlli, sedentari, comparabili per sesso ed età. CRMS Risultati frequenza allelica La distribuzione del genotipo è risultata in accordo con l'equilibrio di Hardy-Weinberg e la frequenza allelica è risultata comparabile nei due gruppi. Non sono state evidenziate differenze significative comparando la distribuzione dei genotipi nei vari tipi di sport. CRMS Athlete’s Heart Distinguishing normal from abnormal • • • • Adeguate Hypertrophy Normal Systolic Function Normal Diastolic Function Reversibility CRMS Athlete’s Heart Distinguishing normal from abnormal • • • • Adeguate Hypertrophy Normal Systolic Function Normal Diastolic Function Reversibility CRMS Types of Myocardial Hypertrophy Normal Adeguate Adeguate NonAdeguate Variability of wall thickness in elite athletes N° Athl Wall Thickness mm Pelliccia.NEJM.1991 Athlete’s Heart Distinguishing normal from abnormal • • • • Adeguate Hypertrophy Normal Systolic Function Normal Diastolic Function Reversibility CRMS Exercise Echocardiography Modifications during Exercise Echocardiography 1. Increse Ejection fraction 2. Decreased Left Systolic Ventricular Volume 3. No significant modifications of Wall Stress CRMS Athlete’s Heart Distinguishing normal from abnormal • • • • Adeguate Hypertrophy Normal Systolic Function Normal Diastolic Function Reversibility CRMS DIASTOLIC FUNCTION IN ATHLETES LVM gr/m2 IVR msec DT msec Ep cm/sec Ap cm/sec ATHLETES 208±28* 69±12* 171±72 84±12* 41±8* CONTROLS 112±21 76±11 203±31 85±19 56±15 Galanti et al, Angiology 1992 4:315-20 Athlete’s Heart Distinguishing normal from abnormal • • • • Adeguate Hypertrophy Normal Systolic Function Normal Diastolic Function Reversibility CRMS Regression of Athlete’s Hypertrophy G.Galanti et al. Cardiologia 1989 Cardiac Adaptation to Exercise chronic Morphological Myocardial hypertrophy •Eccentric •Concentric Coronaries CRMS Coronary Arteries Left Coronary in Athlete Rigth Coronary in Athlete Cardiac Adaptation to Exercise chronic Functional Heart Rate Cardiovascular Response to Acute Exercise in trained subjects H.R. b/min Cycloergometer Recovery