Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
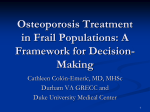
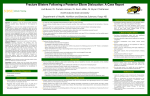
Description of fracture with endocrine therapy use in older breast cancer survivors in a population-based setting Taryn Becker123, Geoff Anderson123, Thiwanka Wijeratne123, Lorraine Lipscombe123, Andrea Gruneir123 , Ophira Ginsburg123, Amy Finch13, Paula Rochon123 1. Women’s College Research Institute 2. Institute for Clinical Evaluative Sciences 3. University of Toronto Background • It is standard practice to treat postmenopausal women with localized hormone-receptor positive breast cancer with adjuvant hormone therapy (HT) • While tamoxifen had been the mainstay of therapy, there is increasing evidence to support aromatase inhibitor (AI) use as the preferred treatment • The 5 year survival among early breast cancer patients is greater than 87% • Increased survival underscores the importance of monitoring for, preventing and treating long term unintended outcomes of HT • AIs are associated with a higher fracture rate compared to tamoxifen. • Clinical trials with over 100 months of follow-up, suggest that the fracture risk is not significant after treatment is completed • However, current evidence is limited: • Highly restricted patient population, which may not be representative of the “real world” • There is an under-representation of older women with increased baseline fracture risk Objectives • To examine the fracture risk in users of hormone therapy • To examine the fracture risk with HT, stratifying by pre-treatment osteoporosis or previous fracture Methods Preliminary Results • . Study design • Overall rates of fracture in the entire cohort were 5.8% for hip fractures and 2.8% for spine fractures 6 • 7992 (85%) prescribed Tamoxifen and 1356 (15%) were prescribed AI • Women in Ontario diagnosed with invasive breast cancer • Diagnosed between April 1, 1996 and March 31, 2006 • The mean (SD) age was 74.8 (6.3) years • Underwent breast cancer surgery within 1 year of diagnosis • Were alive at 365 days from diagnosis • Treatment duration yr (SD): 3.03 (1.55) Median Follow up yr (IQR).: 4.13 (2.29-6.69) • Commenced taking hormone therapy within 1 year of diagnosis 4 3 2 1 Spine • Women aged 66 years and older 5 Hip Study population 7 Fracture Rate (%) • Retrospective population-based cohort design, using administrative databases in Ontario • 9348 women were identified in the cohort 0 Exposure • There were two exposure categories: AI or Tamoxifen started within 1 year of diagnosis Work in Progress Ongoing Analysis • Exposure was based on drug claims from the Ontario Drug Benefit database: • Descriptive statistics among users of tamoxifen and AI • First prescription within 1 year of diagnosis • Patient characteristics, health care usage patterns, pre-existing risk factors for fall and fracture • Second prescription within 150% of days of the first prescription • Relationship between hormonal therapy and fracture Study-specific Dates • Cox proportional hazards regression analysis Maximum Follow-up Date (March 2009) • Stratified analyses by previous fracture or osteoporosis Accrual Window (April 1996-March 2006) Special Considerations Time Look-back Window (up to 5 years) 1 year Observation Window (April 1997- March 2009) Breast cancer diagnosis Outcomes Primary: Fracture • Emergency Room (ER) visit or hospitalization for fracture • Competing risks analysis (death, cancer recurrence) Implications • These data indicate that fractures are common in this population • It is important to further examine which women are at higher risk for fracture, while taking HT as adjuvant therapy for breast cancer. This will help: • Facilitate informed therapy selection • Guide targeted prevention, monitoring, early intervention • Spine, hip, lower extremity, upper extremity, wrist/forearm Acknowledgements We would like to thank Lingsong Yun, Sunila Kalkar, Wei Wu and Peter Anderson for their technical assistance. Excludes: in context of trauma or pathologic fracture This study was conducted with the support of funding provided by the Ontario Institute for Cancer Research and Cancer Care Ontario (through funding provided by the Ministries of Health and Research & Innovation of the Government of Ontario). Follow-up This study is also supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. • Begins 365 days after cancer diagnosis • There is at least a 3-year follow-up allowed for each woman in the cohort • Patients will be followed from diagnosis until the first occurrence of • Fracture • Death • Cancer recurrence or new malignancy • End of follow-up window (March 31, 2009)