Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
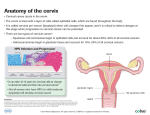
Cervical Cancer and HPV Z Mike Chirenje MD FRCOG University of Zimbabwe, Department of Obstetrics and Gynecology, Harare, Zimbabwe • Summary from (Chirenje ZM, HIV and Cancer of the cervix, in: Best Practice & Research, Clinical Obstetrics and Gynaecology. Vol. 19, No. 2, pp. 269 – 276: April 2005, London UK). Cancer Burden Worldwide • In 1985 it was estimated that there were approximately 7.6 million new cases of cancer diagnosed throughout the world (Parkin DM et al., Int. J. Cancer, 1993) . Cancer Burden in Women • Half of the cases occurred in women • Distribution of cancer is highest in breast followed by cervix • In Africa cervical cancer carries the highest burden occurring in 20-30% cancers among women (compared to 4-6% in high income countries) Cancer Burden in Women • 471,000 new cases diagnosed in 2000 of which 80% were in the developing world • Close to 300,000 women die from cervical cancer worldwide every year • Peak incidence for cervical cancer worldwide is late 40s to early 50s Cervical Cancer Burden by Country Income Country Grouping Estimated Cases, 2002 Percent Share Low income countries of which: India 264,931 (132,082) 54% (27%) Lower middle income 112,232 23% Upper middle income 60,223 12% High Income 54,402 11% Total 491,788 100% Majority of cervical cancer cases are in low income countries Possible target populations: Developing countries: 52.5 million girls High-income countries: 6.5 million girls Source: 2002 Globocan data and PATH staff estimates Estimates of the Number of Cases and Incidence of Cervical Cancer, 2002 Magnitude of Cervical Cancer Problem in Zimbabwean women: Female cancers registered in 2002 by site: • Cervix uteri (771) 25.9% • Kaposi sarcoma (478) 16.1% • Breast (304) 10.2% • Ovary (74) 2.5% • Cervix corpus (40) 1.3% Zimbabwe cancer Registry (2006). • Therefore 1 in every 4 women diagnosed to have cancer had cervical cancer. Epidemiology and Treatment of Cervical Cancer : • Cervical cancer is often slow growing, with progressive generalised wasting for several months that creates difficult home care in low resources. • Family members complain about the unbearable smell that is socially embarrassing and impossible to eradicate (unresponsive to antibiotics). Epidemiology and Treatment of Cervical Cancer : • Survival of cervical cancer patients after treatment in a study by Zimbabwe cancer registry demonstrated that only 26.8% were alive after 3 years (Chokunonga et. al. Int. J. Cancer, 2003). • The peak age for ICC is 46 years resulting in major catastrophic loss for immediate family, community and national economic loss. Epidemiology and Treatment of Cervical Cancer : • Majority (63.3%) are from rural communities • • (Chirenje et. al 2000) where a typical 46 year old woman has 3 to 4 children (oldest 16 years youngest 8 years of age) left behind as young orphans. Majority (80%) present at FIGO > stage 2b Psychological effect on nurses/doctors results in withdrawal/depression symptoms. Cervical Cancer Overview • One of the earliest observations in cancer epidemiology was that cancer of the uterine cervix rarely occurred among celibate nuns (Rigoni-Stern, 1842). Rigoni-Stern D.A, Fatti statistici relativi alle mallattie cancrose. Giovnali per servire ai progressi della Patologia e della Terapeutica (1842); 2: 507 – 517. Role of Screening in advent of HPV Vaccines • The role of oncogenic HPV has been establishes as necessary cause of ICC and its precursor (CIN) • Over 100 different genotypes identified of which 40 detected in anogenital area •HPV and Cervical Specific Lessions HPV infections are among the most common sexually transmitted infections among adults. HR DNA is age dependant (peak age late 20’s) with rates of 15 – 20% and drops significantly to 2-6% by mid thirties when the age specific incidence rates (ASIR) of ICC are peaking up. HPV Epidemiology • Evidence from several African studies demonstrate prevalence of multiple HPV types among women with normal cytology, abnormal cytology, CIN 2/3 (up to 50% HPV types 16, 18) and ICC ( up to 70 % HPV types 16, 18). Persistence of HR HPV infection (16,18,26,31, 33,35,39,45,51,52,53,56,58,59,66,68,73 and 82) is necessary for development, maintenance and progression of CIN the known precursor for ICC. Persistence of HPV DNA from types 16, 18, 45 and 31 are found in 99.7% of all ICC. Studies over the past 15 years have conclusively established that oncogenic HPV types (16, 18, 31, 45) are aetiologically linked to CIN III and invasive cervical cancer. (Womach SD, Chirenje ZM, et al, BJOG 107(1) 33-38, Int.J. Cancer 2000. 85, 206 - 210 • Summary from (Chirenje ZM, HIV and Cancer of the cervix, in: Best Practice & Research, Clinical Obstetrics and Gynaecology. Vol. 19, No. 2, pp. 269 – 276: April 2005, London UK). Practice Points • HIV-positive women have 2 to 12 fold higher risk of CIN lesions compared with HIV-negative women. • HIV positive women should be offered cervical cytology screening, referral for colposcopy and follow-up with 6-monthly cervical cytology surveillance. • Treatment of CIN lesions in HIV-positive women has high recurrence rates, irrespective of treatment modality (Chirenje ZM et al, J. Lower Gen. Tract. Disease 2003).