Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
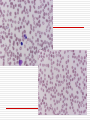
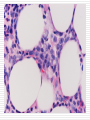
Myelodysplastic Syndromes: Clonal Myeloid Diseases Haskell (Gill) Kirkpatrick M.D. 8/24/05 Case Report 74 y/o man with hx prostate cancer (XRT 2004) and ETOH intake presented with dyspnea Exam pertinent for decreased pallor. No lymphadenopathy or organomegaly. Labs: WBC 1.5, Hct 15, reticulocyte count 1%, platelets 44,000 CD34 CD117 MPO MDS Arise from somatic mutations in hematopoietic (myeloid) stem cell causing: Ineffective hematopoiesis Cytopenia(s) Qualitative disorders of blood cells and their precursors Variable predilection to undergo evolution to florid AML Stem cells have a defective capacity for self-renewal and differentiation History of Terminology “Odo-leukemia” coined in 1942 Disorders on the threshold of leukemia “Pre-leukemic anemia” soon replaced Described cases of cytopenias that preceded the onset of AML “Hemopoietic dysplasia” later shortened to “Myelodysplasia” 1975 conference on unclassifiable leukemias Myelodysplasia: Misnomer Nomenclature coined at a time when Dysmorphogenesis thought to be single abnormality Dysplasia is a pathologic term that implies a non-clonal, non-neoplastic process Encompasses heterogeneous spectrum: From acquired indolent idiopathic anemia… No discernable leukemic blasts To oligoblastic myelogenous leukemia Increased leukemic blast cells (>2%) “refractory anemia with excess blasts” World Health Organization (WHO) Classification FAB criteria introduced in 1982 2001 WHO published new classification scheme Modifications made to improve prognostic value Major changes: Lower threshold for defining AML (Blasts count) Eliminated RA with excess blasts in transformation (RAEBT) Divided categories into single or multi-lineage dysplasia Divided RAEB into 2 categories Eliminated CMML from MDS category Categories not addressed: hypocellular MDS & MDS with fibrosis Incidence and Etiology 15,000 new cases in U.S. annually 5 per 100,000 persons per year Increases to 20 to 50 per 100,000 after the age of 60 As common as CLL (most common form leukemia) Idiopathic Secondary (treatment related) Chemotherapy (particularly alkylating agents) Radiation Clinical Features Asymptomatic Symptomatic anemia Recurrent infections due to granulocytopenia Bleeding due to thrombocytopenia and/or qualitative platelet defect Laboratory features Blood Red cells: Anemia 85% patients at diagnosis MCV often increased Anisocytosis Poikilocytosis: oval, elliptical, teardrop, spherical, fragmented Usually low reticulocyte count Granulocytes and Monocytes Monocytosis and neutropenia not uncommon Pseudo-Pelger-Hüet cells Hypogranular neutrophils Platelets Mild to moderate thrombocytopenia 25% cases Abnormal function assays can reflect qualitative defects Blood Laboratory features Marrow Normal or increased cellularity 20% are hypoplastic Dysplasia in one or more cell line Erythroid hyperplasia and variation in erythroblasts Ringed Sideroblasts: erythroblasts with mitochondrial iron aggregates Hypogranulated neutrophils Unilobed/bilobed megakaryocytes Fibrosis Increase in reticulin and collagen fibers can be seen in oligoblastic leukemia Aspirate Dysplastic RBCs binucleation, multinucleation, nuclear budding, nuclear bridging, karryorhexis, vacuoles, PAS+ Megaloblastoid changes Ringed sideroblasts Macrophage storage Megakaryocytes: Small, hypolobulated nuclei Larger with widely spaced nuclei Morphology: Pitfalls and Problems Morphologic dysplasia not specific for MDS Small number of dysplastic cells can be seen in normal individuals Guidelines (WHO): 10% of cells must be dysplastic in a single lineage Quality of specimen can be an obstacle Make sure adequate staining to call hypogranularity (neutrophils) Biopsies should be at least 1-2 cm extending into marrow Especially with low-grade MDS Studies have shown this especially with dyserythropoiesis Other conditions: megaloblastic anemia, exposure to toxins (i.e. arsenic), congenital dyserythropoietic anemia, growth factors, HIV etc.. Inter-observer reproducibility of dysplasia is poor Cytogenetic Characterization of MDS Role: confirmation of diagnosis & predicting outcome Contributed to understanding of pathogenesis Suspected multi-step process of insults to stem cell genome Routine karyotyping De Novo MDS: Abnormal 40-70% cases Therapy-related (t-MDS): Abnormal 95% cases Predict survival and assess risk of transformation to acute leukemia Often same abnormal chromosomes seen in AML No cytogenetic abnormality specific for MDS One unique case: 5q- syndrome 5Q- Syndrome Deletion of chromosome 5q is one of most common abnormalities in MDS Common deleted region mapped to 5q31q32 (1.5 Mb) “5q- syndrome” Isolated 5q deletion Severe anemia, normal or elevated platelets Atypical megakaryocytes No blasts Typically indolent coarse International Prognostic Scoring System (IPSS) Derived from data from over 800 patients managed with supportive care (Greenberg et al, Blood 1997) Compliments both classification schemes WHO and FAB Morphologic classification alone insufficient Bone Marrow Transplant Allogeneic hematopoetic stem-cell transplant Currently only treatment that can significantly prolong survival Approximately 1/3 of transplanted patients cured Significant morbidity and treatment related mortality Only 8-10% of all MDS patients eligible and have a donor (HLA-matched sibling) Young patients (45 or younger) Therapeutic Goals When Transplant Not an Option Consider natural history of the disease & patient preference Low or Intermediate-1 patients (IPSS): longer survival Principle goal: amelioration of hematologic deficits Need to be durable improvements Int-2/high risk patients: Extending survival becomes more “immediate priority” Prolonging time to development of AML Supportive Care Transfusions Erythropoietin G-CSF If no blasts Targeting Angiogenesis in MDS Angiogenic molecules generated by the neoplastic clone Vascular endothelial growth factor-A (VEGF-A) medullary neovascularity clonal expansion of receptor-competent myeloblasts Ineffective hematopoiesis in receptor naïve progenitors Inflammatory cytokines potentiate ineffective hematopoiesis Small molecule inhibitors of angiogenesis are a potential class of therapeutics Thalidomide Lenalidomide (Revlamid) Thalidomide and MDS Anti-angiogenic and TNFα inhibitory properties Phase II trials done Around 18% response rate (red cell transfusion independence or >50% decrease in transfusion requirement) Non-erythroid lineage improvement uncommon Prolonged treatment necessary for maximal benefit Median interval to response: 16 weeks Side effect profile becomes problematic (i.e. neuropathy) Lenalidomide (Revlimid) Derivative of thalidomide More potent and lacks neurologic toxicities Safety and efficacy trial (List et al NEJM 2/05) RBC transfusion independence with cytogenetic response in 10/12 (83%) patients with del 5q31 Transfusion independence in non-5q patients 39% Sustained > 2years Lenalidomide (Revlimid) Phase II trial (List et al ASCO 5/05) 148 patients Low or intermediate-1 risk (IPSS score) Del 5q isolated (as well as other abnormalities) 66% transfusion independence (median duration > 47 weeks) Cytogenetic response 70% (complete reponse 44%) Myelosuppression common Other Novel Therapeutic Targets: DNA methylation and Epigenetics Addition of a CH3 (methyl) group to a molecule (cytosine base) DNA methyltransferase Epigenetics: Regulation of gene expression without altering DNA sequence Epigenetic silencing Gene promoter regions get methylated Leads to histone modifications Chromatin is remodeled and becomes “invisible” to transcription factors Gene is “silenced” Important role in embryogenesis Thought to be exploited by cancers to help express their malignant phenotype silence tumor-suppressor genes DNA Methylation in MDS Multiple genes known to be hypermethylated/silenced P15 (cyclin dependent kinase inhibitor): frequent target Inactivation associated with risk of progression to AML Associated with disease progression DNA Methylation Inhibitors 5-Azacytidine (AZA) and 5-aza-2’-deoxycytidine (DAC) Cytosine analogs: inhibit DNA methylation by trapping DNA methyltransferases Irreversible bond, degredaded Cells then divide in absence of DNA methyltransferases Dosage key Hypomethylating at low doses, cytotoxic at high doses Maximally tolerated dose (MTD) determined in 70’s Recent low-dose studies show response (and hypomethylation) at 10-30 times lower than MTD Current studies exploring optimal dosing schedules ongoing 5-Azacytidine (Vidaza) Phase III randomized trial (Silverman et al JCO 2002) compared AZA to supportive care Treatment-naïve patients (various stages) 60% response rate (hematologic) that was durable Improved quality of life Prolongation of median time to leukemic transformation or death 21 months vs. 13 months (statistically significant) Not powered for OS and cross-over permitted Sub-cutaneous injection daily X 7 days every 28 days FDA approval 2004 for treatment of MDS Summary MDS represents a group of heterogeneous neoplastic disorders Cytogenetics compliment morphology and help determine prognosis and treatment goals New novel therapies such as 5-Azacytidine (Vidaza) and soon to be approved Lenalidomide (Revlimid) have added options for non-transplant candidates