Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
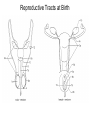
Reproductive System Getting Genes Into The Next Generation Fertilization brings together a haploid sperm and a haploid egg (ovum) to form a diploid zygote and embryo. Haploid Diploid Haploid Diploid Overall Strategies of Reproduction Males Produce haploid gametes (sperm - testes) Produce lubricants and nutrients for sperm (seminal fluids) Deliver semen to female reproductive system (penis) Provide hormones to coordinate system Females Produce haploid gametes (ovaries) Produce lubricants for intercourse Receive semen from male (vagina) Provide for development of embryo (uterus and placenta) Provide nutrients for growth of enfant (breasts – lactation) Provide hormones to coordinate system Basic Male Anatomy Ureter Urinary bladder Seminal Vesicles seminal fluid Prostate gland seminal fluid Penis erectile tissue semen delivery Glans sensitive nerve endings Epididymis store sperm sperm mature/motile Testis (Testes) spermatogenesis endocrine tissue Basic Female Anatomy Uterus Site of embryological development Ureter Urinary Bladder Urethra Clitoris sensitive nerve endings Oviduct (uterine tube) site of fertilization carries sperm to ovum carries embryo to uterus Ovary Oogenesis Endocrine tissue Cervix Vagina separates the uterus accommodates and the vagina the penis Development of Reproductive Organs 1. Undifferentiated gonad 2. Wolffian ducts 3. Mulerian Ducts 4. Ureter 5. Genital tubercle 6. Cloaca 7. and 8. Labioscrotal fold 9. Anus Genetics of Sex • Normally humans have two complete sets of chromosomes: pairs of 23 different chromosomes. • Normally females have two “X” chromosomes and males have a mismatched pair: one “X” and one “Y”. • The Y chromosome carries genes that will help to regulate the normal development of a male embryo/fetus. At 10 weeks of development, visible differences in male and female embryos begin to occur. Genes from the Y chromosome (only present in males) activate the production of testosterone and Mullerian Inhibiting Substance (MIS). These Substances sustain the development of the Wolffian Ducts and inhibit the development of the Mullerian ducts. In the absence of testosterone and MIS, the reproductive tract will develop as a normal female phenotype. Reproductive Tracts at Birth Androgen Insensitivity Syndrome (Testicular Feminizing Syndrome) • Normal XY genotype • Have a mutated gene that codes for the testosterone receptor, and sometimes the MIS receptor as well. • Produce normal levels of testosterone, but the target tissues are unable to respond. • Wolffian ducts do not persist and Mullerian ducts may develop. • If MIS is present, then no uterus will develop and the vagina is small. • Normal female phenotype develops - except, testes are located where the ovaries belong. • Often undetected prior to puberty. • Externally puberty proceeds as normal, but no menstruation occurs. Three Siblings with Androgen Insensitivity Syndrome Male Reproduction Epididymis D C Seminiferous Tubules Testis Spermatogenesis B A Interstitial Cells Of Leydig A and B = Spermatogonia D = Spermatids C= Spermatocyte • Interstitial Cells of Leydig = produce Testosterone. • Sertoli Cells (Sustenacular Cells) Surround spermatocytes and spermatids. Produce Inhibin What Effects Does Testosterone Have? • Normal Embryological Development in Males • Stimulates growth and development of the male reproductive tract at puberty • Stimulates spermatogenesis • Male secondary sex traits (Height, muscle mass, larger larynx, facial and body hair) Inhibits GnRH Secretion Gonadotropic Releasing Hormone GnRH LH + FSH Inhibits FSH secretion Inhibin Physiological Effects Testosterone Role of the Accessory Glands • Seminal Vesicles – fructose (energy source) and prostaglandins that stimulate contractions of female repro. Tract. • Prostate Gland – High pH fluid that neutralizes the acidic environment of the vagina and increases the motility of the sperm. • Bulbourethral gland (Cowper’s Gland) Role of the Scrotum Temperature regulation Female Reproductive System Uterine Tube (oviduct) Myometrium Fimbriae Ovary Endometrium Cervix Vagina Overview of the Menstrual Cycle • Approximately 28 days (may be highly variable) • Day one is counted as the first day after menstrual bleeding stops. • Days 1-14 - Ovum enlargess inside a growing follicle and the endometrial lining of the uterus thickens in preparation to receive a fertilized egg • Day 14 - Ovulation (release of egg from ovary) occurs and the ovum enters the uterine tube. • Days 15-20 – Ovum (or fertilized egg) moves to uterus. • Days 18-21 – If embryo exists, it begins to implant in endometrium • Days 25-28 – If embryo does not implant, endometrial lining as lost in menstrual bleeding. Stages of the Ovarian Cycle GnRH Pre-ovulation Positive Feedback LH + FSH GnRH = gonadotropin Releasing hormone FSH = follicle stimulating hormone LH = luteinizing hormone Low levels of LH and FSH E E 1. The positive feedback of Estrogen at the hypoThalamus causes a surge in GnRH release. GnRH surge 2. The GnRH release causes a surge in FSH and LH FSH and LH Surge 3. The LH surge causes ovulation and the formation of the corpus luteum 4. The Corpus luteum continues to release E and high levels of P 5. The E and P provide negative feedback to the hypothalamus E and P Rising levels of estrogen over several days. Physiological Effects of Estrogen • Estrogen - steroid produced by the ovary *growth of the female reproductive tract *stimulates growth of endometrial lining during each menstrual cycle *stimulates the production of a watery secretion at the cervix. *stimulates breast and hip development and subcutaneous fat layer (secondary sex traits) Physiological Effects of Progesterone • Progesterone * Increases endometrial lining and maintains the endometrial lining. * Causes a thick mucous secretion from the cervix. * Increases the basal metabolic rate (increase in resting body temperature by about 1 degree) If Fertilization Does Not Occur Without additional LH or some other source of hormonal stimulation, the corpus luteum has a limited life; typically around 10 days. After 10 days the corpus luteum will degenerate and turn into scar tissue (corpus albicans). At this point the levels of estrogen and progesterone decline very rapidly. Without estrogen and progesterone, the endometrial lining is lost. Chemical Contraception Birth control pills, Depoprovera (injected 2-4 times per year), and “patches” All contain relatively high levels of estrogen and lower amounts of progesterone. Provides negative feedback to hypothalamus. Interferes with normal secretions of cervix. Fertilization Signaling by the Embryo • Blastocyst • Trophoblast releases Human Chorionic Gonadotropin (HCG) • HCG acts like LH and stimulates the ovary to maintain the corpus luteum • Ovary continues to make progesterone and estrogen. • Endometrial lining is retained - woman “misses her period.”