Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
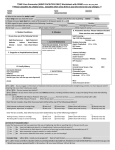
Ambiguous genitalia New term: complex genital anomaly Sex determination Sex differentiation Murran K, Segal D (2009) Disorderd sexual differentiation (Ambiguous genitalia: an appraoch to diagnosis and management. South African Paediatric Review Volume 6 no 3: 20-30 Murran K, Segal D (2009) Disorderd sexual differentiation (Ambiguous genitalia: an appraoch to diagnosis and management. South African Paediatric Review Volume 6 no 3: 20-30 Murran K, Segal D (2009) Disorderd sexual differentiation (Ambiguous genitalia: an appraoch to diagnosis and management. South African Paediatric Review Volume 6 no 3: 20-30 History Clinical Special investigations Detailed family history Prenatal exposure to exogenous or endogenous androgens, estrogens or potential endocrine disruptors Maternal virilization during pregnancy General examination – dysmorphisms Examination of external genitalia Phallus Orifices Labioscrotal folds Gonads Genetics – 46XX, 46XY, 46 XY/X0 Hormones (see cholesterol pathway) 17 OH progesterone DHEA Androstendione Testosterone level Electrolytes Ultrasound Laparoscopy Team approach Family doctor Paediatric endocrinologist Surgeon Geneticist Social worker Psychologist Involve child and parents GENDER ASSIGNMENT Based on - specific pathophysiology prognosis for spontaneous pubertal development potential for sexual activity potential for fertility endocrine function parental wishes Psychosexual development APPROACHES TO GENDER ASSIGNMENT Medical emergency do test stat and inform the parents what the diagnosis is pros and cons Decide gender later and let child decide Decide gender later and child involved in decision Pros and cons Surgical treatment of complex genital anomalies is controversial Specific surgical procedures at specific stages dependent on gender assignment 1. Overvirilization of female fetus (46 XX DSD) 2. Undervirilization of male fetus (46 XY DSD) 3. True hermaphrodite (or ovotesticular DSD) 4. Gonadal dysgenesis Congenital adrenal hyperplasia – not difficult to diagnose Autosomal recessive Leads to deficiency in enzyme function in the cortisol and aldosterone pathways Most common 21 hydroxylase (21OH) deficiency • Girl: - present with ambiguous genitalia - low Na , High K - eventually becomes dehydrated • Boy - presents with dehydration and hyperkalaemia - normal genitalia therefore no clue to diagnosis 46 XY Defect in testosterone production Defect in testosterone metabolism Defect in testosterone action Ovotesticular Disorder of sexual diffirentiation Common in central and southern Africa. Both ovarian and testicular tissue present. Diagnosis confirmed on biopsy of gonads Outcome regarding fertility has been disappointing Spectrum of disorders that lead to the maldevelopment of the gonads and subsequently varying degrees of Disorders of Sexual differentiation Raine J, Donaldson MDC, Gregory JW, Savage MO, Hintz RL (2006) Practical Endocrinology and Diabetes in Children 109-128 Murran K, Segal D (2009) Disorderd sexual differentiation (Ambiguous genitalia: an appraoch to diagnosis and management. South African Paediatric Review Volume 6 no 3: 20-30 Wiersma R True hermaphroditism in southern Africa: the clinical picture Pediatr Surg Int (2004) 20: 363-368 Sperling (2008) Ambiguous genitalia. Paediatric Endocrinology 3rd Edition:127-164