Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
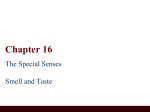
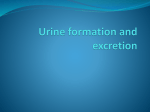
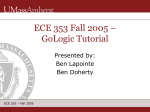
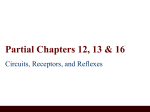
Chapter 23 -2 The Urinary System Basic processes of urine formation LaPointe Spring ‘12 Slide # 2 • Filtration • Blood pressure • Water and solutes across glomerular capillaries • Reabsorption • The removal of water and solutes from the filtrate (95-99% of fluid filtered is reabsorbed) • Secretion • Transport of solutes from the peritubular fluid into the tubular fluid Renal function LaPointe Spring ‘12 Slide # 3 • Most regions of the nephron perform a combination of functions • General functions can be identified as • Filtration in the renal corpuscle • Nutrient reabsorption along the PCT • Ion and water reabsorption along entire nephron and collecting ducts • Active secretion at PCT, DCT, and collecting ducts • Loop of Henle regulates final volume and solute concentration Reabsorption and secretion LaPointe Spring ‘12 Slide # 4 • Accomplished via diffusion, osmosis, and carriermediated transport • Transcellular transport • Substances pass through cells of tubule wall. • Apical membrane: surface that faces filtrate. The lumenal side. • Basolateral membrane: faces interstitial fluid. The sides the part of the cell attached to the basement membrane • Paracellular transport – between the cells Mechanisms of Reabsorption LaPointe Spring ‘12 Slide # 5 Basolateral membrane lumen apical membrane Paracellular transport LaPointe Spring ‘12 Slide # 6 1 2 3 3 H2O 4 solute 1 solute uptake 2 tranport to basolateral space 3 osmotic gradient pulls water in 4 solvent drag brings in more solute Carrier Mediated Transport LaPointe Spring ‘12 Slide # 7 • See chapter 3 • • • • Facilitated diffusion Active transport Cotransport Countertransport • Carrier proteins have a transport maximum (Tm) • Determines renal threshold - plasma concentration of a solute at which it will begin appearing in the urine. Tubular Maximum (Tm) LaPointe Spring ‘12 Slide # 8 Tm renal threshold LaPointe Spring ‘12 Slide # 9 Tubular maximum LaPointe Spring ‘12 Slide # 10 Figure 27-4; Guyton and Hall Overview of Urine Formation LaPointe Spring ‘12 Slide # 11 From Martini Reabsorption and secretion LaPointe Spring ‘12 Slide # 12 • Glomerular filtration produces fluid similar to plasma without proteins • The PCT reabsorbs 60-70% of the filtrate produced • Reabsorption of most organic nutrients (glucose, amino acids, lipids, etc) • Active and passive reabsorption of sodium, bicarbonate, and other ions • Reabsorption of water • Secretion also occurs in the PCT PCT transport systems LaPointe Spring ‘12 Slide # 13 • Glucose and amino acids • Sodium • Bicarbonate • roles of carbonic anhydrase CO2 + H2O H2CO3 • Chloride • Water channels (aquaporins) H+ + HCO3- Transport Activities at the PCT LaPointe Spring ‘12 Slide # 14 Basolateral membrane Apical membrane From Seeley, Stephens and Tate NaHCO3 Reabsorption in the PCT LaPointe Spring ‘12 Slide # 15 From Seeley, Stephens and Tate The loop of Henle LaPointe Spring ‘12 Slide # 16 • Reabsorbs ~50% remaining water and 66% remaining solute (about 15% of the filtered water and 25% of the filtered solute) • Thin segment - concentrates the tubular fluid • Has water channels to reabsorb water • Secretes urea into the tubules • TAL - dilutes the tubular fluid • Transports Na+/K+/2Cl- Na+/K+/2 Cl- cotransport in TAL LaPointe Spring ‘12 Slide # 17 Lasix (furosemide) From Martini Figure 26.13a Reabsorption and secretion at the DCT • DCT performs final adjustment of urine • Active secretion or absorption • Absorption • Tubular cells actively reabsorb Na+ and Cl• In exchange for K+ or H+ (secreted) LaPointe Spring ‘12 Slide # 18 Secretion and Reabsorption at the DCT LaPointe Spring ‘12 Slide # 19 From Martini Figure 26.14 HCO3- + and NH4 transport in the DCT LaPointe Spring ‘12 Slide # 20 From Martini Figure 26.14c Reabsorption and secretion along the collecting ducts LaPointe Spring ‘12 Slide # 21 • Water and solute loss is regulated by aldosterone and ADH • Reabsorption • Sodium ion, bicarbonate (explained in next chapter), and urea • Secretion • hydrogen ions (affected by acid base status as described in next chapter) Cells of the collecting ducts LaPointe Spring ‘12 Slide # 22 • Principle cells • Water channels (aquaporins) • Na + channels • Sodium reabsorption is regulated by aldosterone and water reabsorption is regulated by ADH • Intercalated cells • Mostly secrete H+ in exchange for K+ via an H+ /K+ ATPase similar to the stomach • Also have an H+ ATPase Control of urine volume and osmotic concentration • Final urine volume and osmotic concentration are regulated by controlling water reabsorption in the collecting ducts • Precise control allowed via facultative water reabsorption LaPointe Spring ‘12 Slide # 23 Effects of ADH on DCT & Collecting Ducts LaPointe Spring ‘12 Slide # 24 Figure 26.15a, b Balance and homeostasis LaPointe Spring ‘12 Slide # 25 Osmotic concentrations in the kidney LaPointe Spring ‘12 Slide # 26 Figure 25.13 Countercurrent multiplication LaPointe Spring ‘12 Slide # 27 • Loop of Henle • Functional differences between ascending and descending limbs of loop • Creates osmotic gradient in medulla • Facilitates reabsorption of water and solutes before the DCT • Permits passive reabsorption of water from tubular fluid • Collecting duct reabsorbs urea and sends it back to the descending loop – keeps recycling and thus concentrating the urea Cortical and Juxtamedullary Nephrons LaPointe Spring ‘12 Slide # 28 Urea • Responsible for large part of high osmolality in medulla • Descending limbs of loops of Henle permeable to urea; urea diffuses from the interstitial fluid into the tubule (is secreted) • Ascending limbs and distal tubules are impermeable to urea • Collecting ducts permeable to urea; some diffuses out into interstitial fluid • Urea flows in a cycle maintaining high urea concentration in medulla LaPointe Spring ‘12 Slide # 29 Countercurrent Multiplication and Concentration of Urine Also see Saladin fig 23.20 on slide 32 LaPointe Spring ‘12 Slide # 30 Summary of loop of Henle transport LaPointe Spring ‘12 Slide # 31 From Seeley, Stephens and Tate The Multiplier System (positive feedback) LaPointe Spring ‘12 Slide # 32 Cortical and Juxtamedullary Nephrons LaPointe Spring ‘12 Slide # 33 From Martini Figure 26.7a Summary table LaPointe Spring ‘12 Slide # 34 Sunmmary table continued LaPointe Spring ‘12 Slide # 35 (Also see Fig 23.22 for a great summary of transport across the tubule segments and Table 23.1 for hormonal control of the kidney) The ureters • Pair of muscular tubes • Extend from renal pelvis to the bladder • Peristaltic contractions force urine toward the urinary bladder LaPointe Spring ‘12 Slide # 36 The urinary bladder LaPointe Spring ‘12 Slide # 37 • Hollow, muscular organ • Reservoir for the storage of urine • Contraction of detrusor muscle voids bladder (read book for micturation reflex) • Internal features include • Trigone • Neck • Internal urethral sphincter • Rugae Gross Anatomy of the Urinary Bladder LaPointe Spring ‘12 Slide # 38 Figure 26.19c The urethra LaPointe Spring ‘12 Slide # 39 • Extends from the urinary bladder to the exterior of the body • Passes through external urinary sphincter (urogenital diaphragm) • Differs in length and function in males and females Male transverse section LaPointe Spring ‘12 Slide # 40 From Martini Figure 26.19a Female transverse section LaPointe Spring ‘12 Slide # 41 From Martini Figure 26.19b Composition of normal urine LaPointe Spring ‘12 Slide # 42 • Varies with the metabolic and hormonal events of the body • Reflects filtration, absorption and secretion activity of the nephrons • Urinalysis is the chemical and physical analysis of urine • color • pH (4.5-8.2) • specific gravity (measure of concentration of urine water is 1.000)_ • Protein (not normally present) • glucose (not normally present) • ions, hormones, drugs, etc