Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Ligand binding assay wikipedia , lookup
Gaseous signaling molecules wikipedia , lookup
Metabolomics wikipedia , lookup
Biosynthesis wikipedia , lookup
Surround optical-fiber immunoassay wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Schmerber v. California wikipedia , lookup
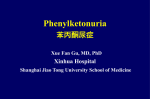
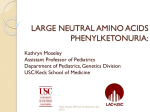
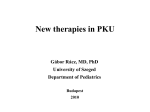
Screening for phenylketonuria (PKU) – laboratory methods Péter Monostori Phe & BH4 metabolism pathway During the hydroxylation of Phe by Phe hydroxylase (PAH) to form tyrosine (Tyr), tetrahydrobiopterin (BH4) is oxidized to a 4a-hydroxy-BH4 intermediate (when molecular oxygen and iron (Fe2+) are present). q-Dihydrobiopterin Phe & BH4 metabolism pathway This intermediate is subsequently regenerated back to BH4 via quinonoid (q)-dihydrobiopterin by the enzymes pterin-carbinolamie4a-dehydratase (PCD) and by the NADH-dependent dihydropteridine reductase (DHPR). Dihydropteridine reductase (DHPR) q-Dihydrobiopterin Pterin-4α-carbinolamine dehydratase (PCD) Phe & BH4 metabolism pathway GTP cyclohydrolase (GTPCH) BH4 is synthesized from guanosine triphosphate (GTP) by three additional enzymes: GTP cyclohydrolase I (GTPCH), 6-pyruvoyltetra-hydropterin synthase (PTPS), and sepiapterin reductase (SR). Mutations in genes Dihydropteridine coding enzymes for reductase (DHPR) 30% GTPCH, PCD, SR, q-Dihydrobiopterin DHPR and PTPS result in BH4 Pterin-4α-carbinolamine deficiency. dehydratase (PCD) 5% 5% 6-Pyruvoyl-tetrahydrobiopterin synthase (PTPS) 60% Sepiapterin reductase (SR) Which markers can be useful in the diagnosis of PKU and BH4 deficiency? PKU: Phe (from DBS) Tyr (DBS) Phe/Tyr ratio (DBS) BH4 deficiency: Neopterin, biopterin and pterin levels (urine, DBS) DHPR activity (DBS) Homovanillic acid (HVA) (liquor) 5-Hydroxy-indoleacetic acid (5-HIAA) (liquor) Definitions of positive/negative predictive value, sensitivity and specificity Sensitivity The proportion of affected subjects that have a positive test result Specificity The proportion of unaffected subjects that have a negative test result Positive predictive value The chance that a positive test result actually indicates an affected individual The proportion of „real” positive samples within all positive results Negative predictive value The chance that a negative test result actually excludes the disorder The proportion of „real” negative samples within all negative results The beginnings… 1920: A child with developmental delay was born to American parents living in China. No one could help in finding the disease. The mother wrote a book, describing the symptoms. The child was later diagnosed as having classical PKU. Overview of the methods for PKU screening – The Folling-test 1. In the 1930s: Asbjorn Folling: a mother noticed a strange smell of her mentally retarded child’s urine → Folling analyzed the urine with various tests including the ferric chloride test (for aromatic hydroxyl groups, such as those in ketones): When ketones are present, urine develops a redbrown colour. This time the urine turned into dark-green. Folling isolated a substance from the urine which was confirmed to be phenylpyruvate. The Folling-test The ferric chloride test (for urine): not sensitive: usually positive at plasma Phe concentrations above 900 μM (dark green coloration) not specific: a slightly altered color reaction may be indicative of other metabolic disorders/medication: maple syrup disease (MSUD) tyrosinemia salicylates, L-DOPA metabolites… traditionally, the reagent was dropped on the diaper of the baby The Guthrie-method 2. From the 1960s: Robert Guthrie and Ada Susi developed a bacterial inhibition assay, suitable for the screening of PKU for the first time. This assay monitors the growth of a mutant strain of Bacillus subtilis with a requirement for exogenous Phe for growth. DBS samples are placed onto agar plates containing mutant bacteria and an inhibitor. The sizes of the colonies are assessed after incubation. The Guthrie-method – principals The growth of Bacillus subtilis is inhibited by an appropriate amount of β-2-thienylalanine added to the agar. This inhibition is reversed when a dried blood spot (DBS) containing the blood of a patient with PKU is placed on the agar → Phe in the blood permits the growth of bacteria around the DBS. The test is positive if the diameter of the growth zone is between the 2 mg% (120 μM) and the 4 mg% (240 μM) standard points (marked). The amount of growth is proportional to the level of Phe in the DBS. The Guthrie-method Standards: 2 4 8 16 32 (mg%) The Guthrie-method Control agar plate without β-2-thienylalanine inhibitor Rationale: antibiotic therapy can prevent the growth of Bacillus subtilis, resulting in false-negative results A new blood sample is obtained if a zone with signs of inhibited bacterial growth is found (marked) The Guthrie-method – characteristics inexpensive specific semiquantitative not very sensitive: limit of detection ≈180-240 μM (=3-4 mg%) Fluorimetric assays 3. From the 1960s: Fluorimetric assays McCaman and Robins (1962): for the determinaton of Phe only principals: the reaction of Phe, ninhydrin and copper yields a weakly fluorescent product the fluorescence is increased by the addition of a dipeptide, L-leucyl-L-alanine Wong, O’Flynn and Inouye (1964): modified the above method to measure Phe, and added another method to determine Tyr Ambrose, Ingerson, Garrettson and Cliung (1967): optimized the Phe-assay by changing several parameters Fluorimetric assays – characteristics quantitative automatization is possible sensitivity is good: of detection may be as low as 6 μM (0.1 mg%) limit not specific (other substances may also yield some degree of fluorescence) Enzymatic colorimetric assays 4. From the 1980s: Enzymatic colorimetric assays Wendel, Hummel and Langenbeck (1989): for the measurement of Phe using dehydrogenase, NAD and a chlorophore Campbell L-phenylalanine et al. (1992): modified the method to reach greater specificity (lower cross-reactivity with Tyr) Enzymatic colorimetric assays – characteristics quantitative automatization is possible sensitivity is acceptable: limit of detection is about 43 μM (0.7 mg%) (higher than that of the fluorescence assay) the specific Liquid chromatography-tandem mass spectrometry (LC-MS/MS) 5. From the 1990s: liquid chromatography- tandem mass spectrometry (LC-MS/MS) allows the simultaneous measurement of a number of disorders of amino acid, organic acid and fatty acid metabolism, including PKU deuterated internal standards are used derivatization with butanol-acetyl chloride is employed selected ratios of the amino acids (or acylcarnitines) are used to help the evaluation LC-MS/MS assays – characteristics quantitative automated rapid very sensitive: lower than 1 μM (0.07 mg%) very specific the false-positive rate is the lowest, highlighting the advantage of using the Phe/Tyr ratio (Tyr levels are simultaneously measured): example: parenteral amino acid supplementation or too much blood on the filter paper: Phe ↑, but Phe/Tyr is normal → PKU can be excluded PKU screening – Blood sampling primary sample: blood spots dried on filter paper (DBS) stability of DBS: ≈10 days at room temperature for amino acids (≈7 days for acylcarnitines) problems associated with blood sampling: inappropriate timing inappropriate technique delayed delivery insufficient data on the patient/parent Problems with blood sampling (DBS) a) Inappropriate timing of blood sampling (rule: 48-72 h of age; earlier: < 5 days) the catabolic state associated with birth is the main trigger of most amino acid (incl. Phe) and acylcarnitine elevations in the first few days of life (and not feeding) (this is not true for galactosaemia and some other disorders) delayed blood sampling may cause false-negative results Problems with blood sampling (DBS) b) Inappropriate technique of blood sampling is mainly responsible for the SD of the MS/MS method insufficient blood excess blood DBS has not dried Safe NOT safe Safe Problems with blood sampling (DBS) c) Delayed delivery of samples d) Insufficient data on the child/parent about drugs, parenteral feeding/glucose/middlechain triglycerides given to the newborn contact address and telephone number of the parent The diagnostic value of Phe assays a positive screening result in a Phe assay is generally sufficient to conclude that some form of hyperphenylalaninemia (PKU, transient hyperphenylalaninemia or BH4 deficiency) is present confirmation by means of genetic testing or gas chromatography-mass spectrometry (GC/MS) is not essential Analysis of PKU with (GC/MS): urine samples Plus: 4-hydroxy-phenyllactate, 4-hydroxy-phenylpyruvate, mandelic acid The diagnostic value of Phe assays (continued) PKU and BH4 deficiency cannot be distinguished from each other by Phe levels plus Phe/Tyr ratios for the differential diagnosis of BH4 deficiency: BH4 loading test, pterin profile analysis (from urine or DBS), dihydropteridine reductase (DHPR) activity measurement (from DBS) should be performed Phe & BH4 metabolism pathway GTP cyclohydrolase (GTPCH) Mutations in genes coding enzymes for BH4 synthesis (GTPCH, PCD, SR), and BH4 recycling (PTPS, DHPR) result in BH4 deficiency. 5% 6-Pyruvoyl-tetrahydrobiopterin synthase (PTPS) 60% Sepiapterin reductase (SR) Dihydropteridine reductase (DHPR) 30% q-Dihydrobiopterin Pterin-4α-carbinolamine dehydratase (PCD) 5% Diagnosis of BH4 deficiency 1. BH4 loading test useful in all forms of BH4 deficiency single Phe dose plus a single BH4 dose 3 h later blood sampling: -3; 0; 4; 8; 12; 16; 24 h (if basal Phe level is low (e.g. < 360 μM), a 24 h Phe loading test may be performed prior to the BH4 test) Diagnosis of BH4 deficiency 2. Analysis of pterins with HPLC plus fluorescent or MS/MS detection Levels of neopterin, biopterin and pterin are measured from urine or DBS. Chromatographic separation is needed. Identifies variants: 65-70% of cases. 3. DHPR activity measurement Primary sample: DBS Identifies a single variant: 30-35% of cases. Pterin levels and DHPR activity in variants of BH4 deficiency Phe (plasma) Biopterin (urine) Neopterin (urine) DHPR activity (blood) Homovanillic acid (HVA, liquor) 5-hydroxyindoleacetic acid (5-HIAA, liquor) GTPCH1 (recessive) N GTPCH1 (dominant) N N ( in liquor) N ( in liquor) N N/ PTPS N PCD N/ primapterin N N N DHPR N SR N N ( in liquor) N ( liquor sepiapterin) N Summary The ideal method for PKU screening is sensitive, specific, rapid and reliable. Of the numerous techniques for the measurement of Phe, the Guthrie method, fluorimetric and enzymatic colorimetric assays, and LC-MS/MS (the most recent technique) are used widely for screening purposes. For the differential diagnosis of hyperphenylalaninemias, BH4 loading test, pterin profile analysis, or measurement of DHPR activity can be performed. Thank you for your attention!