Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
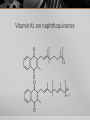
Pharmacogenomics Case study 1: Warfarin Warfarin overview Warfarin is an anticoagulant drug which inhibits vitamin K 2,3-epoxide reductase. Warfarin is used to reduce blood clots and after stroke. The therapeutic index (=LD50/ED50) for warfarin is small. Warfarin is a coumarin, a derviative of dicoumarol, which was discovered in spoiled sweet clover. It was developed by the University of Wisconsin. The name is derived from Wisconsin Alumni Research Foundation coumarin. Similar drugs are acenocoumarol and phenprocoumon. Warfarin action is affected by both pharmacodynamics and pharmacokinetics Variations in Vitamin K epoxide reductase could result in more or less inhibition by warfarin. Variations in vitamin K dependent carboxylase could also affect warfarin activity. Variability in CYP450 2C9 and 3A4 will affect metabolism. The Vitamin K cycle Vitamin K is required for formation of γcarboxyGlu A number of proteins are known to contain γ-carboxyGlu residues. These include blood coagulation factors II (prothrombin), VII, IX, and X, the anticoagulant proteins C and S, and the Factor Xtargeting protein Z. This modification is necessary for blood clotting. γ-CarboxyGlu is made in a post-translational modification requiring vitamin K. Vitamin Ks are naphthoquinones The proposed mechanism of vitamin K dependent carboxylase Does Vitamin K dependent Glu carboxylase affect warfarin response ? A number of polymorphisms of GGCX have been identified. Most of these are in the non-coding regions. One mutation, R325Q, is found in the coding region. R325Q has about 30% higher activity than “wild-type”. These mutations were found to have only a modest effect (6- 10%) on the warfarin dose. No crystal structure of this endoplasmic reticulum associated protein has been obtained. Question? Vitamin K dependent Glu carboxylase is not the target of warfarin. Why could it affect warfarin activity? Recycling of vitamin K After carboxylation, vitamin K is in the oxidized epoxide form. It needs to be reduced back to the hydroquinone for the next cycle of carboxylation. This is done by vitamin K 2,3-epoxide reductase. This enzyme is the target of warfarin inhibition. A bacterial analogue structure of vitamin K reductase The quinone binding site The proposed reduction sequence A possible mechanism for vitamin K epoxide reduction Polymorphisms in VKOR Polymorphism Daily Warfarin Dose mg Resistance Phenotype Wild type 4–6 A41S 16 Moderate R58G 34 Major V66M 31 Major L28R >45 Severe V45A Target INR never Severe Reached Common SNPs in noncoding regions 1–15 Variations across the “normal” dosing range Many of these mutations are at or near the quinone binding site Location of mutations known to affect warfarin binding Stereochemistry of warfarin inhibition of VKOR The activity of the two enantiomers towards VKOR differs, with S-warfarin being 3–5 times more potent than R-warfarin. Warfarin is a racemic mixture. Thus, S-Warfarin accounts for approximately 70% of the overall anticoagulant activity. Warfarin resistance has also appeared in animals Warfarin has been used as rodent poison for about 50 years. However, resistance has developed in rats and mice. These rodents show polymorphism in VKOR. Resistance may be due at least in part to VKOR polymorphisms. Mouse polymorphisms in VKOR Geographic Amino acid area substitutions No. of samples Berlin E37G 12 Lower Saxony E37G 1 R58G 13 Westphalia R12W, A26S, A48T, R58G, R61L R12W, A26S, A48T, R61L Rhineland Azores L128S 7 2 17 Y139C 1 Y139C 1 How do the mutations in rats and mice compare with humans? Most of the the mutations in rats and mice are different than those is humans. However, the mutations occur in the same regions of the protein, positions 29 to 48 in exon 1, positions 58 to 67 in exon 2, and 120 to 143 in exon 3. It is unclear if the mutations in VKOR are solely responsible for resistance in rodents. Most of the mutations result in reduced enzyme activity. Question? Why do all of the mutations found in VKOR result in weaker rather than stronger warfarin binding? What other enzyme(s) could contribute to warfarin resistance? Question? What are some other drugs that should not be used with warfarin?