Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
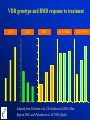
Pharmacogenetics of response to antiresorptive therapy: Vitamin D receptor gene Tuan V. Nguyen, Associate Professor John A. Eisman, Professor and Director Bone and Mineral Research Program Garvan Institute of Medical Research Sydney, Australia Osteoporosis heterogenous pathophysiological mechanisms and response to therapy Variability in BMD = 0.12 x Mean Variability in DBMD = 3 x Mean Variability in response to therapy: 1-3 x Mean DBMD 5 450 Alendronate Placebo Probability of density (%) 400 No. of subjects 350 300 250 200 150 100 4 3 2 1 50 0 0 -14 -12 -10 -6 -4 -2 0 2 4 6 9 17 -40 Rate of change (%/year) Nguyen et al, JBMR 1999 Average rate of BMD loss: -0.6 1.8 %/yr -30 -20 -10 0 10 20 30 Percent change in lumbar spine BMD Adapted from Cummings et al, JAMA 1998 40 Individual vs average Clinical – efficacy and tolerance – Duration – new pharmacologic targets Theoretical – genetics of BMD – genetics of BMD change – environmental factors Available data genetic polymorphisms and response to antiresorptive therapy Genetics of BMD and body composition rMZ rDZ H2 (%) Lumar spine BMD 0.74 (0.06) 0.48 (0.10) 77.8 Femoral neck BMD 0.73 (0.06) 0.47 (0.11) 76.4 Total body BMD 0.80 (0.05) 0.48 (0.10) 78.6 Lean mass 0.72 (0.06) 0.32 (0.12) 83.5 Fat mass 0.62 (0.08) 0.30 (0.12) 64.8 Nguyen, et al, Am J Epidemiol 1998 VDR genotype and BMD • VDR genotype and osteocalcin levels (PNAS, 1992) • VDR genotype and BMD (Nature, 1994) • Contentious association • Meta-analysis: 15 cross-sectional, cohort studies • Bayesian modelling VDR genotype and lumbar spine BMD Melhus H et al. Melhus H et al. Kroger H et al. Kroger H et al. Riggs BL et al. Riggs BL et al. Berg JP et al. Berg JP et al. Boschictsch et al. Boschictsch et al. Garneo P et al. Garneo P et al. Jorgensen HL et al. Jorgensen HL et al. Kiel et al. Kiel et al. McClure L et al. McClure L et al. Vandevyver C et al. Vandevyver C et al. Gennari L et al. Gennari L et al. Hansen TS et al. Hansen TS et al. Gornez C et al. Gornez C et al. Langdahl BL et al. Langdahl BL et al. Marc J et al. Marc J et al. Overall Overall -2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0 Effect size (bb vs BB) 1.5 2.0 -1.0 -0.5 0.0 0.5 Effect size (bb vs Bb) 1.0 1.5 Pooled effects of VDR genotype on BMD: Bayesian analysis bb - BB bb - Bb 4.0 7 3.5 Probability of density (%) Probability of density (%) 6 3.0 2.5 2.0 1.5 P |d >0| = 0.940 1.0 0.5 5 4 3 2 P |d > 0| = 0.80 1 0.0 -0.03 -0.02 -0.01 0.00 0.01 0.02 0.03 0.04 0.05 0.06 0.07 0 -0.02 Absolute difference in lumbar spine BMD between bb and BB (g/cm2) Overall difference: 14.7 (95% CI: 0.8 to 42.3) mg/cm2 -0.01 0.00 0.01 0.02 0.03 0.04 Absolute difference in lumbar spine BMD between bb and Bb (g/cm2) Overall difference: 5.8 (95% CI: -6.5 to 18.0) mg/cm2 BsmI b allele associated with higher BMD Model of drug response Activity of other biological systems Drug effect Target responsiveness Drug concentration at target Drug response Adverse reaction Drug concentration at other biological systems Responsiveness at other biological systems Other predisposition Adapted from Meisel, et al. J Mol Med 2003 Heritability of BMD change • 21 MZ and 19 DZ twin pairs over 3 years • Changes in lumbar spine BMD: rMZ = 0.93 vs rDZ = 0.51 (Kelly et al. JBMR 1993; 8:11-7) • 25 MZ and 21 DZ male twin pairs over 14 years • Changes in distal radius BMD: rMZ=0.61, rDZ=0.41 (NS) (Christian, et al. 1989) VDR genotype and BMD change Significant association No significant association Rapuri, J Steroid Biochem & Mol Biol 2004 Gunnes, JCEM 1997 Garnero, JBMR 1996 Hansen, Bone 1998 Gomez, Osteoporosis Int 1999 Guardiola, Ann Int Med 1999 Gough, J Rheumatol 1998 Publication bias? Deng, Hum Genet 1998 Zmuda, JBMR 1997 Ferrari, Lancet 1995 Krall, JBMR 1995 In “positive” studies, BsmI b allele associated with lesser loss or greater increase in BMD Inter-subject variability in response to antiresorptive therapy 5 Alendronate Probability of density (%) Placebo 4 3 2 1 0 -40 -30 -20 -10 0 10 20 30 40 Percent change in lumbar spine BMD Adapted from Cummings et al, JAMA 1998 Placebo: n=2218, mean change in LSBMD: 1.5 ± 8.1 % Alendronate: n=2214, mean change in LSBMD: 8.3 ± 7.8 % Pharmacogenetics of response to antiresorptive treatments • Few studies • Candidate gene approach VDR genotypes and response to Raloxifene Rx BMD Bone turnover markers n=66 osteoporotic women; duration of Rx: 1 yr Palomba et al. Human Reprod 2003; 18:192-8 VDR genotypes and response to Alendronate Rx BMD Bone turnover markers n=68 osteoporotic women; duration of Rx: 1 yr Palomba et al. Clin Endocrinol 2003; 58:365-71 VDR genotype and BMD response to treatment ALN RLX HRT 9 9 8 8 7 7 ALN+RLX ALN+HRT 9 9 8 8 7 7 6 6 5 5 4 4 3 3 2 2 6 6 5 5 4 4 3 3 2 2 1 1 0 0 BB Bb bb BB Bb bb 1 1 BB Bb bb Adapted from Palomba et al. Clin Endocrinol 2003; Hum Reprod 2003; and Palomba et al, OI 2005 (Epub). BB Bb bb Genetic factors and response to antiresorptive therapy • Response to antiresorptive therapy is multifactorial (VDR genotypes explained 5-10% of the variability) • SNPs profile could allow individualization of treatment • Issues of study design and interpretation Bayesian decision approach SNP association studies: Bayesian approach to decision Alternatives 1. Abandon study 2. Continue data collection 3. Evidence strong enough for molecular exploration Rationale for decision True positive assoc. / False positive assoc. = 20/1 (NOT the same as p-value) A hypothetical scenario • 20 SNPs (out of 1000 SNPs) are actually associated with BMD response to Rx • Study power = 80% (i.e., type II error = 20%) • Type I error = 5% • Finding: Significant association for 1 SNP (P = 0.05) • What is the probability that there is indeed an association? 20 SNPs involved; Power = 80%; False +ve = 5% 1000 SNPs Association (n=20) a=5% power=80% Significant N=16 No association (n=980) Nonsignificant Significant (n=49) Nonsignificant True positive / False positive = 16/49 P(True association | Significant result) = 16/(16+49) = 25% The need for lower P-value About 25% of all findings with “p<0.05” should, if viewed in a scientifically agnostic light, properly be regarded as nothing more than chance findings (1). • Proportion of significant associations depends on: – p-value, – overall proportion of hypotheses being tested are true – statistical power • For a ratio (true +ve) / (false +ve) association = 20:1, p-value should be lowered by 400 times • For a ratio (true +ve) / (false +ve) association = 50:1, p-value should be lowered by 1000 times (1) J Berger (1987); R Matthews (2001) Bayesian resolution of conflicting finding Change in LSBMD in response to ALN Rx: bb vs BB genotypes Probability density 0.25 0.20 0.15 Current data (D=-4.6%, Var=6.7) 0.10 Marc OI 1999 0.05 P(bb-BB>3%) = 0.01 0.00 0.25 0.20 Prior distribution (D=4.1%, Var=0.4) 0.15 0.10 Palomba 2003, 2005 P(bb-BB>3%) = 0.91 0.05 0.00 0.25 0.20 Posterior distribution (D=3.6%, Var=0.37) 0.15 0.10 P(bb-BB>3%) = 0.73 0.05 0.00 -20 -15 -10 -5 0 5 10 15 20 Genetic markers could allow identification of those more or less likely to – fracture – respond to a specific treatment – suffer side effects from a specific treatment With cost-benefits in relation to intervention, Bayesian method offers a powerful approach to individualise inference Acknowledgments Nguyen D. Nguyen Garvan Institute of Medical Research Regia Congressi Organizing C’tee Reserved slides Misunderstanding of P-value Bisphosphonate treatment was associated with a 5% increase in BMD compared to placebo (p<0.05) 1. It has been proved that bisphosphonate is better than placebo? 2. If the treatment has no effect, there is less than a 5% chance of obtaining such result 3. The observed effect is so large that there is less than 5% chance that the treatment is no better than placebo 4. I don’t know 60 52 50 Percent 40 30 20 19 15 15 10 0 1 2 Answer 3 4 1. Better treatment; 2. <5% chance of getting the result if there is no effect; 3. <5% due to chance 4. I don’t know (Source: Wulff et al., Stat Med 1987; 6:3-10) P value is NOT • the likelihood that findings are due to chance • the probability that the null hypothesis is true given the data • P-value is 0.05, so there is 95% chance that a real difference exists • With low p-value (p < 0.001) the finding must be true • The lower p-value, the stronger the evidence for an effect P-value • Grew out of quality control during WWII • Question: the true frequency of bad bullets is 1%, what is the chance of finding 4 or more bad bullets if we test 100 bullets? • Answer: With some maths (binomial theorem), p=2% So, p-value is the probability of getting a result as extreme (or more extreme) than the observed value given an hypothesis Process of Reasoning The current process of hypothesis testing is a “proof by contradiction” If the null hypothesis is true, then the observations are unlikely. If Tuan has hypertension, then he is unlikely to have pheochromocytoma. The observations occurred Tuan has pheochromocytoma ______________________________________ ______________________________________ Therefore, the null hypothesis is unlikely Therefore, Tuan is unlikely to have hypertension What do we want to know? • Clinical P(+ve | Diseased): probability of a +ve test given that the patient has the disease P(Diseased | +ve): probability of that the patient has the disease given that he has a +ve test • Research P(Significant test | No association): probability that the test is significant given that there is no association P(Association | Significant test): probability that there is an association given that the test statistic is significant Diagnostic and statistical reasoning Diagnosis Research Absence of disease There is no real difference Presence of disease There is a difference Positive test result Statistical significance Negative test result Statistical non-significance Sensitivity (true positive rate) Power (1-b) False positive rate P-value Prior probability of disease (prevalence) Positive predictive value Prior probability of research hypothesis Bayesian probability For a given sample size, posterior probability increases with p-value 1.0 Posterior Probability of Association 0.9 p = 0.0001 p = 0.001 0.8 0.7 0.6 0.5 p = 0.01 p = 0.05 0.4 0.3 0.2 0.1 0.0 0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 Prior Probability of Association 0.8 0.9 1.0 50 18 50 16 50 14 50 12 50 10 0 85 0 65 0 45 25 0 160 140 120 100 80 60 40 20 0 50 Number of studies Distribution of sample sizes Sample size Ioannidis et al, Trends Mol Med 2003 Distribution of effect sizes 100 80 60 40 20 4 8 2. 2. 2 6 1. 8 0. 1. 2 5 0. 0 0 Number of studies 120 Effect size (OR) Ioannidis et al, Trends Mol Med 2003 Correlation between the odds ratio in the first studies and in subsequent studies Ioannidis et al, Nat Genet 2001 Evolution of the strength of an association as more information is accumulated Ioannidis et al, Nat Genet 2001 Predictors of statistically significant discrepancies between the first and subsequent studies of the same genetic association Odds ratio – univariate analysis Predictor Odds ratio – multivariate analysis Total no. of studies (per association) 1.17 (1.03, 1.33) 1.18 (1.02, 1.37) Sample size of the first study 0.42 (0.17, 0.98) 0.44 (0.19, 0.99) Single first study with clear genetic effect 9.33 (1.01, 86.3) NS Ioannidis et al, Nat Genet 2001