Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
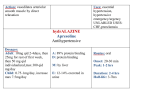
They all died of bacterial infections or sequelae - antibiotics could have or would have been used King Tut – Staphylococcus aureus Beth March – Streptococcus pyogenes Pope John Paul II - Sepsis Common Antibiotics Original Power Point by Nicole Morse B.Pharm MSHP Updated by Jennifer Wong B.Pharm, GCPC Pharmacists, Cabrini Health Overview • • • • • Aminoglycosides Beta-lactams Vancomycin Clindamycin Macrolides Metronidazole Quinolones Rifampicin Tetracyclines Aminoglycosides • Gentamicin – Broad Gm-ve spectrum, incl. Ps.aeruginosa – D.O.C for most cases of aerobic Gm-ve sepsis • Amikacin – Reserve for organisms resistant to other aminog. • Tobramycin – Marginally more effective on Ps.aeruginosa than gentamicin • All potentially ototoxic and nephrotoxic • C/I with NM-blocking agents paralysis Aminoglycoside - Gentamicin Not absorbed after oral administration Must be admin parenterally to tx systemic infns Eliminated almost entirely by glomerular filtration T1/2 ~2hr (normal pt) Traditional tds dosing Endocarditis, pregnancy, burns, CF Once daily (extended interval) admin the norm Higher concmore rapid & greater bacterial killing Resistance less likely with higher conc PAE Less frequent peaks reduce nephrotoxicity Narrow Therapeutic Margin Aminoglycoside - Gentamicin • Extended interval dosing – 3-4mg/kg (healthy, normal adults) – Post-levels are done 30’ after end of infusion – Pre-levels are done just prior to next infusion • Usually administered over 30’ infusion • Target – Peak 10-12g/mL – Trough <2 g/mL • If post is / you adjust the dose (peak) • If pre is extend the interval (trough) Beta-lactams • Penicillins – Narrow-spectrum • gm+ve, X by -lactamases • PenicillinG iv, PenicillinV po – Narrow spectrum with antistaph activity • Stable to -lactamases • Dicloxacillin, flucloxacillin – Moderate spectrum • Amoxycillin, ampicillin • Also active against some gm-ve – Broad spectrum • Augmentin Duo Forte® Augmentin Duo • Piperacillin and Ticarcillin have activity against P.aeruginosa Beta-lactams con’t • Carbapenems – – – – Imipenem/cilstatin, meropenem, ertapenem New doripenem (Doribax®) Gm-ve rods, P.aeruginosa, anaerobes, many gm+ve Not useful for MRSA • Cephalosporins – Less sensitive to penicillinases – Same spectrum as the penicillins – Have ‘generations’ that indicate broadening spectrum of activity • Commonly you will see: – Cephalothin 1g iv QID (or cephtazidime 1g iv tds) post surgery followed by cephalexin 500mg po QID – Ceftriaxone 1g iv daily with roxithromycin for empirical tx of pneumonia – Ceftriaxone 2g bd or 4g daily could be indicated for empirical treatment of meningitis Regarding penicillin hypersensitivity… 10% of patients who are allergic to penicillins will be allergic to other beta-lactamases and vice-versa “A hx of an immediate hypersensitivity reaction…contraindicates use of other beta-lactams”. Vancomycin • Effective against a broad range of gram +ve organisms, not gram –ve organisms. • Role in MRSA (not VRE) • Role in severe infections with susceptible organisms in pt allergic to penicillin and in meningitis due to Strep.pneumoniae • Not absorbed orally - For systemic infections give iv • Could be given orally for treatment of Clostridium difficile • Vancomycin TDM: – Aim for trough 10mg-20mg/L sampled immediately before the next dose is administered – Peak levels are commonly done but have not been proven to correlate with toxicity or efficacy – Peak levels should be 25mg-40mg/L; values outside this indicate an abnormal Vd and dose adjustment is required. Clindamycin • Used in skin infections and patients allergic to penicillins. • Both iv and oral • Commonly 150mg-300mg tds-qid • Major s/e risk is pseudomembranous colitis!! – Due to overgrowth of Clostridium difficile • VERY important to warn the pt of diarrhea (esp mucousy/bloody/watery) to cease and call the doctor immediately. Macrolides • Azithromycin, Roxithromycin, Erythromycin, Clarithromycin • Cyp3A4 inhibitor interactions increasing along the line • Community acquired infections are major indications • Roxithromycin 150mg po bd or 300mg po d • Erythromycin 250mg po 30ac qid or Erythromycin Ethylsuccinate 400mg swallowed whole qid irrespective of food. Metronidazole • Covers anaerobes • Available as iv but excellent po absorption means tabs/supps can often be used instead. • Disulfiram-like reaction with alcohol • Common rx are 400mg po tds and 500mg iv tds or bd • Abdominal, pelvic, oral infections • Can give mouth a furry metallic taste and a black coating – Both benign and reversible after ceasing therapy Quinolones Reduce dose in renal impairment Broad spectrum – Resistance is increasing, esp in USA • Norfloxacin 400mg bd oral • Ciprofloxacin 500mg bd oral – Also available iv • C/I in children and adolescents •A/E: photosensitivity, dizziness, confusion •Tendon (and bone) damage •Many drug interactions •Prolong the QT inverval Rifampicin • Active against gm+ve – Including Staph & mycobacteria • Used in: TB, MRSA, prophylaxis Hib and meningococcal • Rapid emergence of resistance means it must always be used in combo with another abx (e.g. + fusidic acid is often seen) • Potent CYP450 inducer – Many drug interactions • Colours body fluids yellow-orange Tetracyclines • Broad spectrum – Gm+ve and gm-ve, Chlamydia, spirochaetes et.al. • Resistance and development of other abx has reduced their value • Main use is acne, CAP, PID, cholera, lyme disease • C/I in children under 8y.o & pregnant & breastfeeding women – Staining of teeth and bones • Doxycycline is a blood schizonticide – Used for malaria prophylaxis Questions??? Quiz Name a penicillin Ampicillin, Benzylpeniciliin (PenG), Phenoxymethypenicillin (PenV), amoxycillin, flucloxacillin, dicloxacillin Name two side effects of gentamicin Nephrotoxicity, ototoxicity Which of these is potentially reversible? Nephrotoxicity Who should we not give tetracyclines to? Children under eight years old; pregnant women; breastfeeding women Name a quinolone Ciprofloxacin, norfloxacin, moxifloxacin, gatifloxacin References • Prof Gregory Peterson, UTas, UMORE • Therapeutic Guidelines, Antibiotics • Karen Wong B.Pharm, The Alfred • Rang HP, Dale MM, Ritter JM. 1999. Pharmacology (4th ed.) Churchill Livingstone: Sydney. • Wikipedia