Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
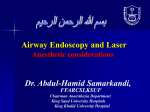
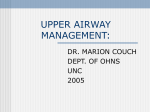
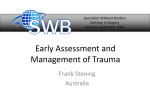
Pediatric Prehospital Airway Management By: Aaron Mills 11/26/07 The Pediatric Airway Introduction Anatomy / Physiology Positioning Adjuncts Intubation Introduction Almost all pediatric “codes” are of respiratory origin As few as 10% of emergency calls involve a peds patient, of which only 1% involve a critically ill or injured child. Reasons Why These Airways Are Difficult Emotional Response Different Anatomy Structures not fully developed Large tongue Pediatric Cardiopulmonary Arrests 10% 10% Respiratory Shock Cardiac 80% Anatomy Children are much harder to intubate than adults Anatomy: Larynx Narrowest point = cricoid cartilage Airway Difference Airway Positioning “Sniffing Position” Towel is placed under the head Airway positioning for children <2yrs Adjuncts Nasal airway Oral airway Nasopharyngeal Airway Contraindications: Basilar skull fracture CSF leak Adjuncts: Oral Airway Wrong size: Too Long Adjuncts: Oral Airway Wrong size: Too Short Adjuncts: Oral Airway Correct size Adjuncts: Oral Airway The importance of proper size Signs of Respiratory Distress Tachypnea Tachycardia Grunting Stridor Head bobbing Flaring Inability to lie down Agitation Retractions Access muscles Wheezing Sweating Prolonged expiration Apnea Cyanosis Intubation Intubation: Indications Failure to oxygenate Failure to remove CO2 Neuromuscular weakness CNS failure Cardiovascular failure Laryngoscope Blades Macintosh Miller Using The Miller Blade Better in younger children with a floppy epiglottis Straight Laryngoscope Blade – used to pick up the epiglottis ET Tube sizes Age Newborn 3 mos 1 yr 2 yrs kg 3.5 6.0 10 12 Children > 2 years: ETT size: ETT depth (lip): ETT 3.5 3.5 4.0 4.5 Length (lip) 9 10 11 12 Age/4 + 4 Age/2 + 12 Predicting the Difficult Airway Difficulty ventilating Facial trauma Obesity Obstructions Stiff lungs (asthma) Difficulty intubating External factors (obesity) Evaluate mouth opening Obstruction Smaller airways Neck mobility (trauma) Easy or Hard? Easy or Hard? Easy or Hard? Back-up Plan Can’t ventilate or basics not working Consider adjuncts (OPA/NPA/positioning) Intubation? Can’t intubate Rescue devices Can’t rescue Surgical procedure Okay to stick with basics if working Overview Anatomy / Physiology Positioning Adjuncts Intubation Questions? References Hazinski MF, et al (Ed). PALS provider manual. AHA, 2005. Lee BS, et al. Pediatric airway management. Clin Ped Emerg Med. 2001. 2(2): 91-106. Lubitz DS. A rapid method of estimating weight and resuscitation drug doses from length in the pediatric age group. Ann Emerg Med. 1998. 17(6):576-581. www.emsresponder.com