Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
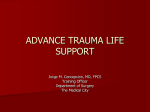
Management of the trauma patient Dr. Zoltan Peto 2010. The Need Trauma is the leading cause of death in the first 4 decades of life in most developed countries. 3.8 million deaths / year worldwide 312 million injured / year worldwide 3 patients permanently disabled / death ACS Trimodal Death Distribution ATLS Concept ● ABCDE approach to evaluation and treatment ● Treat greatest threat to life first ● Definitive diagnosis not immediately important ● Time is of the essence ● Do no further harm ● Good recordkeeping is paramonunt! ATLS Concept Airway with c-spine protection Breathing / ventilation / oxygenation Circulation: stop the bleeding! Disability / neurological status Expose / Environment / body temperature Initial Assessment / Management Injury Transfer Primary Survey Adjuncts Resuscitation Optimize patient status Reevaluation Reevaluation Detailed Secondary Survey Adjuncts Standard Precautions ● Cap ● Gown ● Gloves ● Mask ● Shoe covers ● Goggles / face shield Initial Assessment Primary survey and resuscitation of vital functions are done simultaneously using a team approach. Concepts of Initial Assessment Primary Survey Adjuncts Definitive Care Resuscitation Reevaluation Reevaluation Detailed Secondary Survey Adjuncts Quick Assessment What is a quick, simple way to assess a patient in 10 seconds? ● Identify yourself ● Ask the patient his or her name ● Ask the patient what happened Primary Survey Airway with c-spine protection Breathing with adequate oxygenation Circulation with hemorrhage control Disability Exposure / Environment The priorities are the same for all patients. Primary Survey Exposure / Environment Completely undress the patient Caution Prevent hypothermia Pitfalls Missed injuries Resuscitation ● Protect and secure airway ● Ventilate and oxygenate ● Stop the bleeding! ● Vigorous shock therapy ● Protect from hypothermia Adjuncts to Primary Survey Vital signs ABGs ECG PRIMARY SURVEY Urinary output Urinary / gastric catheters unless contraindicated Pulse oximeter and CO2 Adjuncts to Primary Survey Diagnostic Tools Adjuncts to Primary Survey Diagnostic Tools ● FAST ● DPL Adjuncts to Primary Survey Consider Early Transfer ● Use time before transfer for resuscitation ● Do not delay transfer for diagnostic tests What is the secondary survey? The complete history and physical examination Airway and Ventilatory Management Airway Assessment Signs and symptoms of airway compromise High index of suspicion Change in voice / sore throat Noisy breathing (snoring and stridor) Dyspnea and agitation Tachypnea Abnormal breathing pattern Low oxygen saturation (late sign) Airway Assessment When to intervene when the airway is patent ● Inability to protect the airway ● Impending airway compromise ● Need for ventilation Airway Assessment Impending Airway Obstruction Airway Management ● Supplemental oxygen ● Basic techniques ● Basic adjuncts ● Definitive airway ● ● ● Cuffed tube in the trachea Rapid sequence induction with C-spine protection! Difficult airway adjuncts: Unexpected/Predicted difficult airway Airway Management Definitive Airway ● Surgical airway ● Cricothyroidotomy Needle Surgical Airway Decision Scheme What is shock? Generalized State of Hypoperfusion Inadequate oxygen delivery Catecholamines and other responses Anaerobic metabolism Cellular dysfunction Cell death Signs of shock ● Alteration in level of consciousness, anxiety ● Cold, diaphoretic skin ● Tachycardia ● Tachypnea, shallow respirations ● Hypotension ● Decreased urinary output Shock Hypovolemic ● Blood loss ● Fluid loss vs Nonhemorrhagic ● Tension pneumothorax ● Cardiac tamponade ● Cardiogenic ● Septic ● Neurogenic Interventions What can I do about it? Direct pressure / tourniquet Reduce pelvic volume Angioembolization STOP the bleeding! Splint fractures Operation Interventions What can I do about it? ● Fluid resuscitation ● Vascular access? ● Type? ● Volume? ● Monitor response ● Prevent hypothermia! Class I Hemorrhage 750 mL BVL (15%) ● Slightly anxious ● Normal blood pressure ● Heart rate < 100 / min ● Respirations 14-20 / min ● Urinary output 30 mL / hour Crystalloid Class II Hemorrhage 750-1500 mL BVL (15-30%) ● Anxious ● Normal blood pressure ● Heart rate > 100 / min ● Decreased pulse pressure ● Respirations 20-30 / min ● Urinary output 20-30 mL / hour Crystalloid, ? blood Class III Hemorrhage 1500-2000 mL BVL (30-40%) ● Confused, anxious ● Decreased blood pressure ● Heart rate > 120 / min ● Decreased pulse pressure ● Respirations 30-40 / min ● Urinary output 5-15 mL / hour Crystalloid, blood components, operation Class IV Hemorrhage >2000 mL BVL (>40%) ● Confused, lethargic ● Hypotension ● Heart rate > 140 / min ● Decreased pulse pressure ● Respirations >35 / min ● Urinary output negligible Definitive control, blood components Abdominal Injury When should you suspect abdominal injury? Blunt Penetrating ● Speed ● Weapon ● Point of impact ● Distance ● Intrusion ● Number and location of wounds ● Safety devices ● Position ● Ejection Abdominal Injury Assessment: Physical Exam ● Inspection ● Auscultation ● Percussion ● Palpation Abdominal Injury Factors that Compromise the Exam ● Alcohol and other drugs ● Injury to brain, spinal cord ● Injury to ribs, spine, pelvis Caution A missed abdominal injury can cause a preventable death. Adjuncts X-ray Studies ● Blunt: AP chest and pelvis ● Penetrating: AP chest and abdomen with markers (if hemodynamically normal) Adjuncts Contrast Studies ● Abdominal CT ● Urethrogram ● Cystogram ● IVP ● GI studies Caution Don’t delay definitive care! Laparotomy Indications for Laparotomy – Blunt Trauma ● Hemodynamically abnormal with suspected abdominal injury (DPL / FAST) ● Free air ● Diaphragmatic rupture ● Peritonitis ● Positive CT Laparotomy Indications for Laparotomy – Penetrating Trauma ● Hemodynamically abnormal ● Peritonitis ● Evisceration ● Positive DPL, FAST, or CT Early operation is usually the best strategy for GSW Pelvic Fractures Assessment of Pelvic Fractures ● Inspection ● Leg-length discrepancy, external rotation ● Open or closed ● Palpation of pelvic ring, stability ● Rectal / GU / vaginal exam ● Open or closed? Palpate prostate Thoracic Trauma ● Significant cause of mortality ● Blunt: < 10% require operation ● Penetrating: 15-30% require operation ● Majority: Require simple procedures ● Most life-threatening injuries are identified during the primary survey Thoracic Trauma What are the immediately life-threatening chest injuries? ● Laryngeotracheal injury / Airway obstruction ● Tension pneumothorax ● Open pneumothorax ● Flail chest and pulmonary contusion ● Massive hemothorax ● Cardiac tamponade Thoracic Trauma What are the pathophysiologic consequences of these chest injuries? ● Hypoxia ● Hypoventilation ● Acidosis ● Respiratory ● Metabolic ● Inadequate tissue perfusion Manage in the primary survey as identified Tension Pneumothorax ● Clinical diagnosis, not by x-ray ● Immediate decompression ● Needle ● Chest tube Open Pneumothorax ● 3-sided cover over defect ● Chest tube ● Definitive operation Flail Chest and Pulmonary Contusion Massive Hemothorax ● Systemic / pulmonary vessel disruption ● > 1500 mL blood loss ● Flat vs. distended neck veins ● Shock with no breath sounds and/or percussion dullness Cardiac Tamponade ● Decreased arterial pressure ● Distended neck veins ● Muffled heart sounds ● Pulseless electrical activity Radio antenna Cardiac Tamponade A Secure airway B Ventilate and oxygenate C Volume resuscitation FAST, operation Resuscitative Thoracotomy When should I consider resuscitative thoracotomy? ● Patients with penetrating thoracic injury arriving with PEA may be a candidate ● When a surgeon with appropriate skills is present ● ED thoracotomy not indicated in blunt trauma with PEA Head injury Monro-Kellie Doctrine Volume-Pressure Curve Autoregulation ● If autoregulation is intact, CBF is maintained constant between a mean BP of 50 to 160 mm Hg. ● In moderate or severe brain injury, autoregulation is impaired so CBF varies with mean BP. ● The injured brain is more vulnerable to episodes of hypotension, causing secondary brain injury. Mild Brain Injury ● ● ● ● ● ● ● GCS score = 13 – 15 History Exclude systemic injuries Neurologic exam X-rays as indicated Alcohol / drug screens as indicated Liberal use of head CT Observe or discharge based on findings Moderate Brain Injury ● GCS score = 9 – 12 ● Initial evaluation same as for mild injury ● CT scan for all ● Admit and observe ● ● Frequent neurologic exams ● Repeat CT scan Deterioration: Manage as severe head injury Severe Brain Injury ● GCS score = 3 – 8 ● Evaluate and resuscitate ● Intubate for airway protection ● Focused neurologic exam ● Frequent reevaluation ● Identify associated injuries Indications for CT Scan High Risk ● GCS score still < 15 two hours after injury ● Neurologic deficit ● Open skull fracture ● Sign of basal skull fracture ● Extremes of age Indications for CT Scan Moderate Risk ● “Dangerous mechanism” ● Retrograde amnesia > 30 minutes in duration ● Severe headache ● Vomiting > 2 episodes Management Priorities ● ABCDE ● Minimize secondary brain injury ● Administer oxygen ● Maintain adequate ventilation ● Maintain blood pressure (systolic > 90 mm Hg) Management Focused Neurological Exam ● GCS score ● Pupils ● Lateralizing signs Consult neurosurgeon early Management Medical ● Controlled ventilation ● Goal: Paco2 at 35 mm Hg ● Intravenous fluids ● Euvolemia ● Isotonic ● Consult with neurosurgeon ● Mannitol ● Use with signs of tentorial herniation ● Dose: 0.25 to 1.0 g / kg IV bolus Management Medical ● Other medications ● Anticonvulsants ● Sedation ● Paralytics Neurological examination before prolonged sedation / paralysis Management Surgical ● Scalp Wounds ● Possible site of major blood loss ● Direct pressure to control bleeding ● Occasional temporary closure Management Surgical Scalp Wounds: Possible site of major blood loss Direct pressure to control bleeding ● Intracranial Mass Lesion ● Can be life-threatening if expanding rapidly ● Immediate neurosurgical consult ● Hyperventilation / mannitol ● Damage control craniotomy: transfer to neurosurgeon (rural / austere areas) Anaesthesia of the trauma patient Continue ABCDE in the theatre Apply monitoring: IABP, ECG, SatO2, Temperarure, UOP, Airway gases, etc. Beware of hypovolaemia – reduced amount of drugs needed Beware of reduced amount of drugs – awareness Beware of hypothermia Intensive care after operation Good recordkeeping is paramonunt! Intensive care Standard intensive care monitoring Abdominal pressure monitoring Fracture site/wound awareness ABCDE to be continued Weaning starts with the ventilation Early tracheostomy if needed Respiratory / circulatory / renal support Fluid replacement / blood products therapy Stabilisation on ICU might be the step before operation Intensive care Proper pain relief to be given (opioids) Proper sedation to be given (short acting drugs) Pressure sore prevention Gastric ulcer prevention Thrombosis prophylaxis (LMWH) Antibiotics if indicated Early feeding (preferably enteral feeding) Relatives to be kept informed Good recordkeeping is paramount! ©ACS