Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
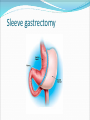
Davaei .M. MD. FACS The Obesity Epidemic 66% of Americans >20 yrs are either overweight or obese (BMI > 25, ~ 133 million people) Increased from 45% in 1960 33% of Americans >20 yrs are obese (BMI > 30, ~ 66 million) 5% of Americans are morbidly obese (BMI > 40, ~ 10 million) 3.1% in men and 6.7% in women Increasing by 1% per year Obesity is increasing in children (doubled in past 20 years) 15% between the age of 6 and 19 NHANES (2003-04) (n=4,431) Body Mass Index (BMI) BMI = weight (kg) / height (m)2 Normal Weight (BMI 18.5 to 24.9) Overweight (BMI 25 to 29.9) Obese (BMI 30 to 34.9) Severely Obese (BMI 35 to 39.9 ) Morbidly Obese (BMI > 40) Super Obese (BMI > 50) Why do we treat obesity?? • Co-morbidities • Quality of life • Survival – Life Expectancy Rationale for Surgery Long Term Outcome Data Sustained Weight Loss Improvement or Resolution of Co-morbidities Improved long term survival Minimally Invasive Surgery Public Awareness Obesity as a disease Celebrities Life Expectancy 2nd only to smoking as the leading cause of preventable death in the United States.† > 110,000 deaths/year in the US are associated with obesity* * Flegal KM et al. JAMA. 2005 Apr 20;293(15):1861-7. † CDC Life Expectancy Potential Consequences of Obesity Obesity is associated with a rise in many comorbid conditions, including: Type 2 Diabetes Hyperlipidemia Hypertension Obstructive Sleep Apnea Heart Disease Stroke Asthma Back and lower extremity weightbearing degenerative problems Cancer Depression AND MORE! Trends In Surgery 1992 - 2003 Who Is a Surgical Candidate? Meets NIH criteria No endocrine cause of obesity Acceptable operative risk Understands surgery and risks Absence of drug or alcohol problem No uncontrolled psychological conditions Consensus after bariatric team evaluation: Surgeon/Dietician/Psychologist/Consultant Dedicated to life-style change and follow-up CONTRAINDICATIONS Untreated major depression or psychosis Binge eating disorders Current drug and alcohol abuse Severe cardiac disease with prohibitive anesthetic risks Severe coagulopathy Inability to comply with nutritional requirements including life-long vitamin replacement Weight Loss Program Team Surgeon Nurse Practicioner Bariatric Coordinator Registered Dietician Clinical psychologist Exercise Specialist Office support staff Preoperative Evaluation/Education Staff evaluation Internist Dietitian Psychologist Nurse Surgeon Support group •Laboratory evaluation – Blood – ECG, CXR – Stress Test – Sleep study – EGD – PFTs Consider an IVC filter for any patient with prior history of DVT/PE. Types of bariatric procedures Restrictive Vertical banded gastroplasty Laparoscopic adjustable gastric band Sleeve gastrectomy Malabsorptive Jejunoileal bypass Biliopancreatic diversion Biliopancreatic diversion with duodenal switch Combination of restrictive and malabsorptive Roux-en-Y gastric bypass VERTICAL BANDING from American Family Physician, 2006, 73(8): 1405. LAP ADJUSTABLE BANDING from American Family Physician, 2006, 73(8): 1405. Sleeve gastrectomy Jejunoileal Bypass Payne and Dewind, Archives of Surgery, 1973 BPD & BPD w/ DUODENAL SWITCH from www.utdol.com:Surgical Options for Obesity. 2006. ROUX-EN-Y GASTRIC BYPASS from American Family Physician, 2006, 73(8): 1404. INTRAGASTRIC BALLOON from www.obezitecerrahisi.com POST-OP COMPLICATIONS Phase I: one to six weeks Phase II: seven to twelve weeks Phase III: thirteen wks to 12 months Overall operative mortality = 1% POST-OP COMPLICATIONS: PHASE I Medical: -pulmonary embolism (1%) -myocardial infarction -respiratory failure -pneumonia -urinary tract infection Surgical: -anastomotic leak (2-3%) -postop bleeding -bowel perforation -bowel obstruction -wound infections POST-OP COMPLICATIONS PHASE II RESTRICTIVE: -staple line disruption or band erosion -stomal stenosis -pouch/esophageal dilatation -port failure -GERD/ulcers -infection (foreign body) ROUX-EN-Y: -gastric remnant distention perf -stomal stenosis -wound infection -cholelithiasis -ventral hernia -incisional hernia POST-OP COMPLICATIONS PHASE III -GERD/esophagitis/gastritis -small bowel obstruction -staple/band erosion -dehydration due to severe constipation or freq vomiting سپاسگزارم