Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
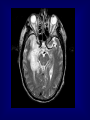
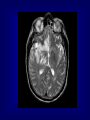
HERPES SIMPLEX ENCEPHALITIS M.RASOOLINEJAD, MD DEPARTMENT OF INFECTIOUS DISEASE TEHRAN UNIVERCITY OF MEDICAL SCIENCE HERPES SIMPLEX ENCEPHALITIS ( HSE ) A SERIOUS ILLNESS WITH SIGNIFICANT RISKS OF MORBIDITY & MORTALITY TREATABLE ENCEPHALITIS EPIDEMIOLOGY Incidence: 1/ 250,000 to 500,000/ year Morbidity: Untreated patients, 70% Treated patients, 19% Morbidity: > 50% of survivors are left with moderate or severe neurologic deficits Sex: In male & female is equal Age: Peaks in childhood & middle-aged HSE Acute or Subacute Illness General & Focal Cerebral Dysfunction Sporadic Without Seasonal Pattern HSV-1 in 95% cases PATHOGENESIS Children & young adult: Primary HSV infection Olfactory bulb Adult: Prior HSV-1 infection ( Ab +ve ) Reactivation in Trigeminal or Autonomic roots Brain Brain PATHOLOGY Edema & Congestion & Hemorrhage &Necrosis Intense Hemorrhagic necrosis In Temporal & Frontal lobe Hallmark of HSE: Bilateral Asymmetrical Anterior Temporal lobe inflammation CLINICAL MANIFESTATIONS NO PATHOGNOMONIC CLINICAL FINDING Typical symptoms: •Fever 90% •Headache 81% •Psychiatrics symptoms 71% •Seizures 67% •Vomiting 46% •Focal weakness 33% •Memory loss 24% •Altered mental status & photophobia CLINICAL MANIFESTATIONS NO PATHOGNOMONIC CLINICAL FINDING Typical finding on P/E: •Alteration of consciousness 97% •Fever 92% •Dysphasia 76% •Seizures 38% (Focal 28%, General 10%) •Hemiparesis 38% •Cranial nerve defect 32% •Visual field loss 14% •Papilledema 14% DIFFERENTIAL DIAGNOSIS Brain abscess Epidural & Subdural abscess Neoplasms, Brain Pediatric febrile seizures Stroke & Hemorrhagic or Ischemic WORK-UP Lab Studies: CSF Mononuclear pleocytosis Elevated protein Nl or reduce glucose Initial may be Nl Hemorrhagic natureElevated RBC HSV is rarely cultured CSF/PCRSensitive & Specific WORK-UP Imaging Studies: MRI ( Preferred mainly imaging ) Bilateral Temporal & Inferior Frontal Changes CT-Scan ( much less sensitive than Other tests: EEG Focal abnormalities MRI ) Slow-wave or periodic sharp-wave Over temporal lobe Sensitive Not Specific TREATMENT Goals of therapy: 1.Shorten the clinical course 2.To prevent complications 1.To prevent subsequent recurrence TREATMENT ASYCLOVIR The drug of choice 10mg/kg (or 500mg/m2 ) IV q8h Each dose infused over 1 hour Duration: 10 to 14 days