Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
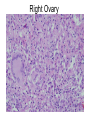
Clinical Pathological Conference May 11, 2007 CHIEF COMPLAINT: 51 year old female with abdominal bloating, twenty pound weight loss, and fatigue for 2 months. DEFENDING DIAGNOSES • • • • Ovarian Carcinoma (9): David Jacobs Krukenberg Tumor (1): Daniel Shen Pelvic Tuberculosis (3): Vanessa Starr Pancreatic adenocarcinoma (1): Jeremy Fenton • Other Diagnoses: Meig’s syndrome Antiphospholipid syndrome Pseudomyxoma Peritonei RADIOLOGY Dr. Michael Macari Associate Professor, Department of Radiology Pelvic Ultrasound Pelvic Ultrasound FACULTY DISCUSSANT Dr. David Chong Associate Program Director Assistant Professor of Medicine, Pulmonary Disease PATHOLOGY Dr. Jian-jun Wei Assistant Professor, Department of Pathology Right Ovary Right Ovary Right Ovary Right Peritoneum Right Peritoneum Right Peritoneum Right Iliac Lymph Node Right Iliac Lymph Node Right Iliac Lymph Node FINAL DIAGNOSIS • Pathologic Diagnosis: Non-caseating Granulomas • Presumed Clinical Diagnosis: Tuberculosis of the Female Genital Tract Hospital Course and Follow-up • The patient had a GI and GYN workup for malignancy. • Her EGD showed: – Normal esophagus. Atrophic mucosa in antrum. Normal dudodenum. – Negative Helicobacter pylori. – Pathology: chronic mildly active gastritis with extensive metaplasia. Hospital course and Follow-up • The patient had an exploratory laparotomy – Evidence of miliary disease – Bilateral oopherectomy and hysterectomy – Pathology: Non-caseating granulomas. (AFB -) • Tuberculosis versus Sarcoidosis • 6 month course of IRPE 6 given for presumed tuberculosis of the female genital tract Epidemiology of Tuberculosis of the Genital Tract • Common in underdeveloped nations • Most affected woman are in the reproductive age-group • In Guyana*, – 900 new cases of active tb per year – estimated annual rate of infection is 3.2% – estimated 14% of the population is infected *World TB report 2005 Pathogenesis of Miliary Tuberculosis Bacilli in the air (droplet nuclei) inhaled Replication in dependant lobe: primary focus Early lymphohematogenous spread Latent Foci TB lymphadentis, Miliary Tuberculosis Clinical Presentation and laboratory data of Tuberculosis of the Genital Tract • • • • • • Abdominal pain Pelvic pain Ascites Diarrhea Infertility Weight loss • Amenorrhea or irregular menses • Fever • Anemia • Elevated CA-125 Making the Diagnosis of Tuberculosis of the Genital Tract • Laparoscopically directed biopsy • Premenstrual endometrial tissue biopsy • Histologic and PCR tests of peritoneal fluid, menstrual blood culture • Exploratory laparotomy Radiographic Features of Tuberculosis Treatment of Tuberculosis of the Genital Tract • Similar to treatment for TB at extrapulmonary sites. • A 6-mo regimen – 2 months of isoniazid, rifampin, and pyrazinamide – 4 months of isoniazid and rifampin – Ethambutol should be used until the results of drug susceptibility studies are available, unless there is little possibility of drug resistance Thank you • • • • • • Medical Students Dr. Macari Dr. Chong Dr. Wei Dr. Grieco Dr. Blaser